

The roles of genetic polymorphisms and human immunodeficiency virus infection in lipid metabolism
- PMID: 24319689
- PMCID: PMC3844249
- DOI: 10.1155/2013/836790
The roles of genetic polymorphisms and human immunodeficiency virus infection in lipid metabolism
Abstract
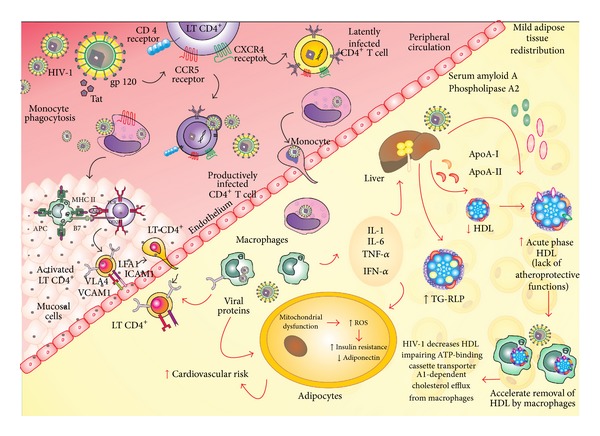
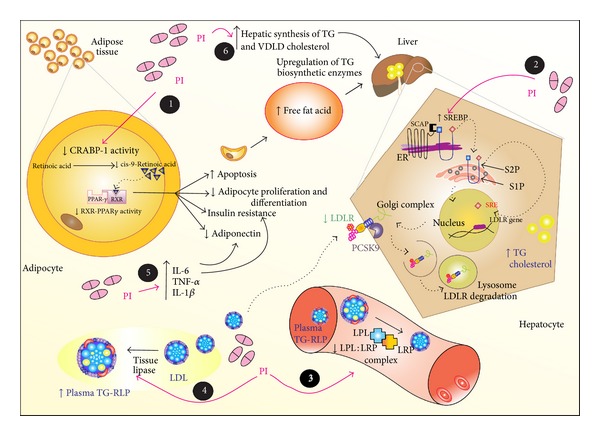
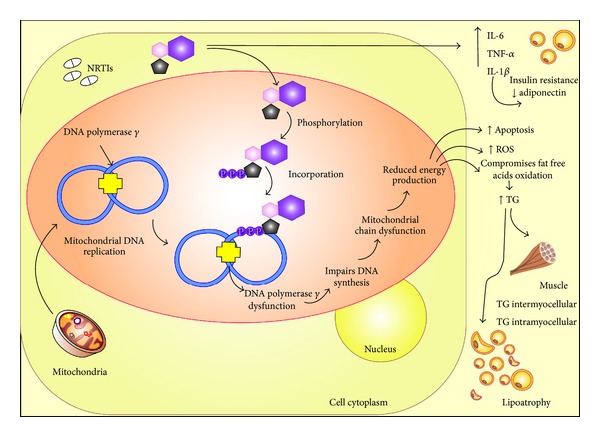
Dyslipidemia has been frequently observed among individuals infected with human immunodeficiency virus type 1 (HIV-1), and factors related to HIV-1, the host, and antiretroviral therapy (ART) are involved in this phenomenon. This study reviews the roles of genetic polymorphisms, HIV-1 infection, and highly active antiretroviral therapy (HAART) in lipid metabolism. Lipid abnormalities can vary according to the HAART regimen, such as those with protease inhibitors (PIs). However, genetic factors may also be involved in dyslipidemia because not all patients receiving the same HAART regimen and with comparable demographic, virological, and immunological characteristics develop variations in the lipid profile. Polymorphisms in a large number of genes are involved in the synthesis of structural proteins, and enzymes related to lipid metabolism account for variations in the lipid profile of each individual. As some genetic polymorphisms may cause dyslipidemia, these allele variants should be investigated in HIV-1-infected patients to identify individuals with an increased risk of developing dyslipidemia during treatment with HAART, particularly during therapy with PIs. This knowledge may guide individualized treatment decisions and lead to the development of new therapeutic targets for the treatment of dyslipidemia in these patients.
Figures
References
-
- Andrade FM, Hutz MH. O componente genético da determinação dos lipídeos séricos. Ciência & Saúde Coletiva. 2002;7(1):175–182.
-
- Valente AM, Reis AF, Machado DM, Succi RC, Chacra AR. Alterações metabólicas da síndrome lipodistrofia do HIV. Arquivos Brasileiros de Endocrinologia & Metabologia. 2005;49(6):10–17. - PubMed
-
- Estrada V, Portilla J. Dyslipidemia related to antiretroviral therapy. AIDS Reviews. 2011;13(1):49–56. - PubMed
-
- Wlodawer A, Vondrasek J. Terapia anti-aids. Annual Review of Biophysics and Biomolecular Structure. 1998;27(249):10–16. - PubMed
-
- Menéndez-Arias L. Molecular basis of human immunodeficiency virus type 1 drug resistance: overview and recent developments. Antiviral Research. 2013;98(1):93–120. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
