

Pulmonary lobe segmentation based on ridge surface sampling and shape model fitting
- PMID: 24320514
- PMCID: PMC3843757
- DOI: 10.1118/1.4828782
Pulmonary lobe segmentation based on ridge surface sampling and shape model fitting
Abstract
Purpose: Performing lobe-based quantitative analysis of the lung in computed tomography (CT) scans can assist in efforts to better characterize complex diseases such as chronic obstructive pulmonary disease (COPD). While airways and vessels can help to indicate the location of lobe boundaries, segmentations of these structures are not always available, so methods to define the lobes in the absence of these structures are desirable.
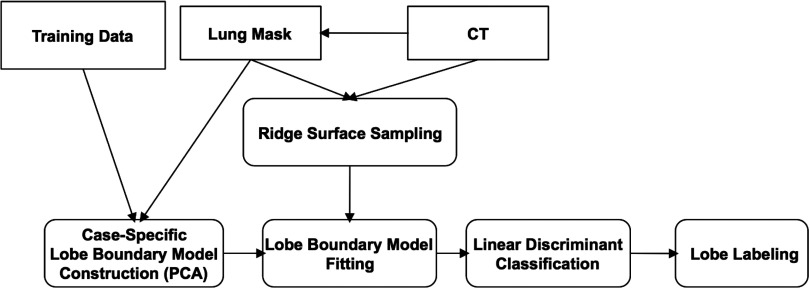
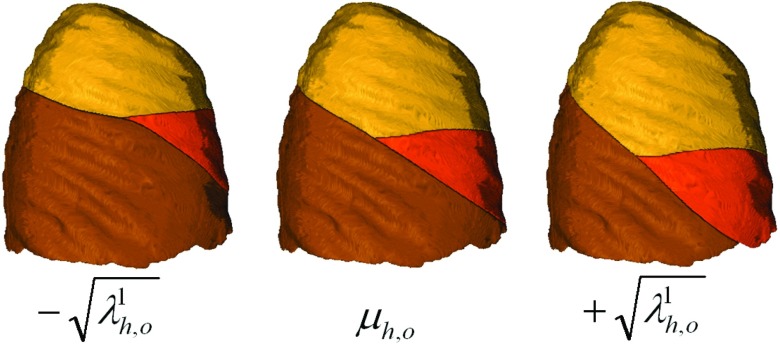
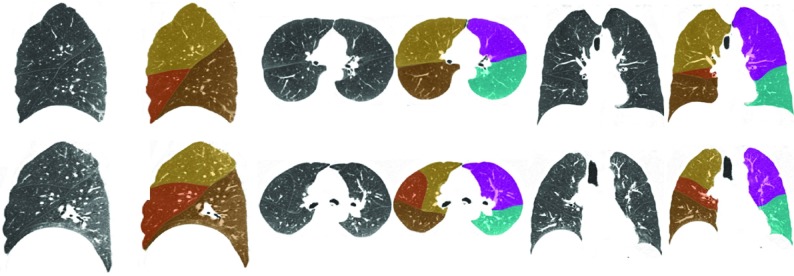
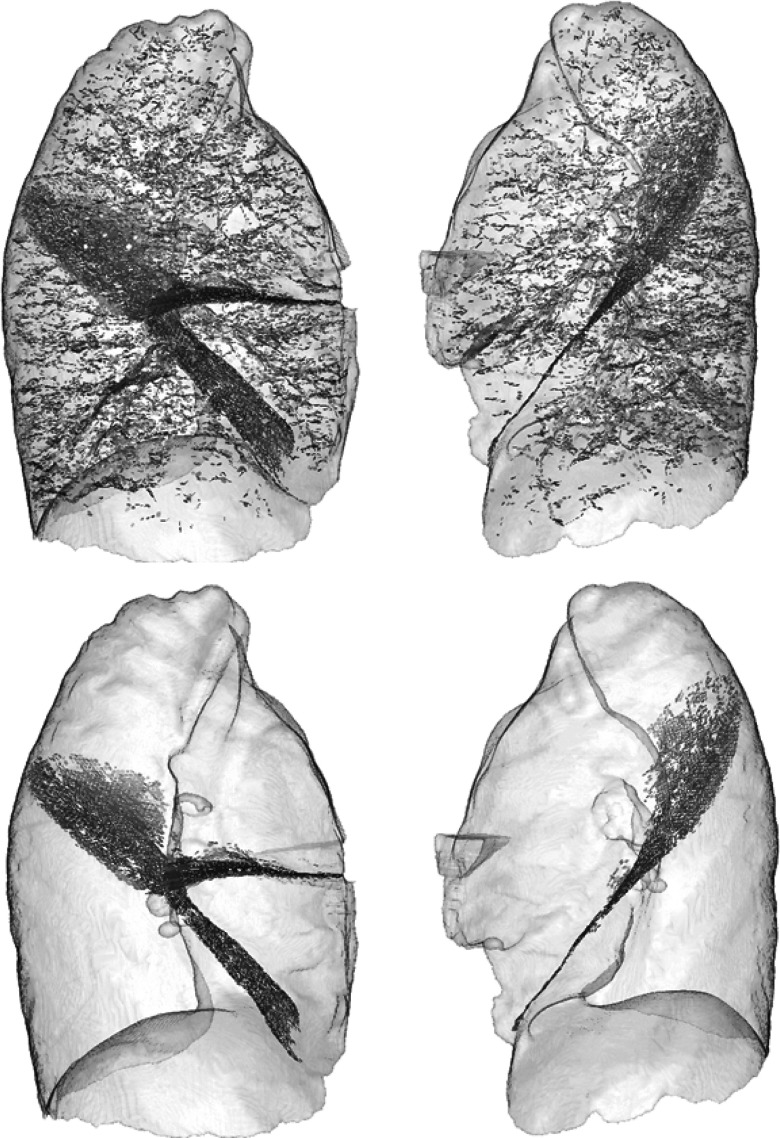
Methods: The authors present a fully automatic lung lobe segmentation algorithm that is effective in volumetric inspiratory and expiratory computed tomography (CT) datasets. The authors rely on ridge surface image features indicating fissure locations and a novel approach to modeling shape variation in the surfaces defining the lobe boundaries. The authors employ a particle system that efficiently samples ridge surfaces in the image domain and provides a set of candidate fissure locations based on the Hessian matrix. Following this, lobe boundary shape models generated from principal component analysis (PCA) are fit to the particles data to discriminate between fissure and nonfissure candidates. The resulting set of particle points are used to fit thin plate spline (TPS) interpolating surfaces to form the final boundaries between the lung lobes.
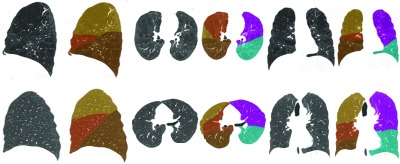
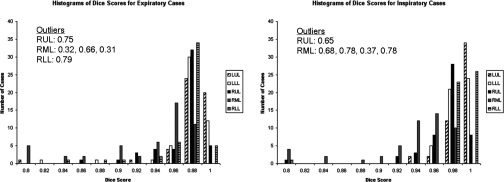
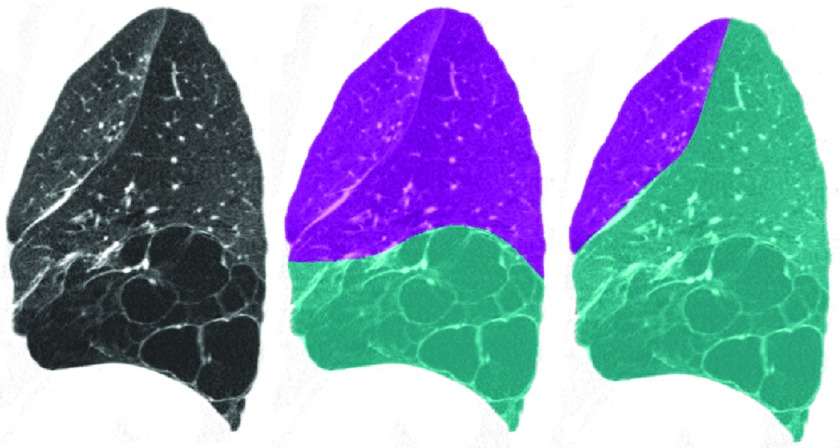
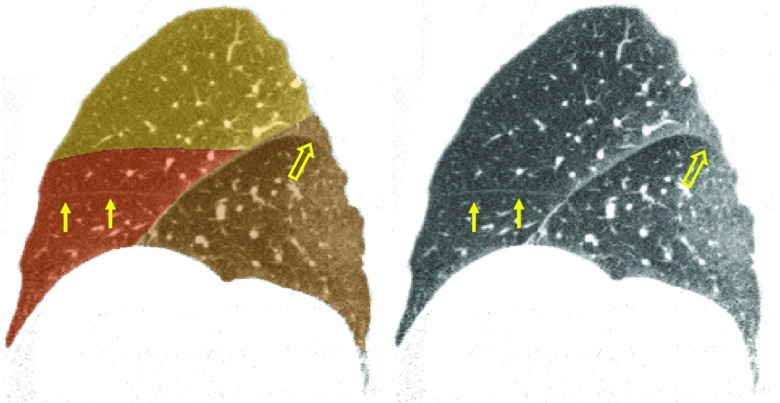
Results: The authors tested algorithm performance on 50 inspiratory and 50 expiratory CT scans taken from the COPDGene study. Results indicate that the authors' algorithm performs comparably to pulmonologist-generated lung lobe segmentations and can produce good results in cases with accessory fissures, incomplete fissures, advanced emphysema, and low dose acquisition protocols. Dice scores indicate that only 29 out of 500 (5.85%) lobes showed Dice scores lower than 0.9. Two different approaches for evaluating lobe boundary surface discrepancies were applied and indicate that algorithm boundary identification is most accurate in the vicinity of fissures detectable on CT.
Conclusions: The proposed algorithm is effective for lung lobe segmentation in absence of auxiliary structures such as vessels and airways. The most challenging cases are those with mostly incomplete, absent, or near-absent fissures and in cases with poorly revealed fissures due to high image noise. However, the authors observe good performance even in the majority of these cases.
Figures


Similar articles
-
Automatic lung lobe segmentation using particles, thin plate splines, and maximum a posteriori estimation.Med Image Comput Comput Assist Interv. 2010;13(Pt 3):163-71. doi: 10.1007/978-3-642-15711-0_21. Med Image Comput Comput Assist Interv. 2010. PMID: 20879396 Free PMC article.
-
Automatic pulmonary fissure detection and lobe segmentation in CT chest images.Biomed Eng Online. 2014 May 7;13:59. doi: 10.1186/1475-925X-13-59. Biomed Eng Online. 2014. PMID: 24886031 Free PMC article.
-
Validation of automated lobe segmentation on paired inspiratory-expiratory chest CT in 8-14 year-old children with cystic fibrosis.PLoS One. 2018 Apr 9;13(4):e0194557. doi: 10.1371/journal.pone.0194557. eCollection 2018. PLoS One. 2018. PMID: 29630630 Free PMC article.
-
Volumetric expiratory HRCT of the lung: clinical applications.Radiol Clin North Am. 2010 Jan;48(1):177-83. doi: 10.1016/j.rcl.2009.09.003. Radiol Clin North Am. 2010. PMID: 19995635 Review.
-
A pulmonary nodule mislocated in "dorsal" segment due to tri-lobed left lung.Front Surg. 2023 Jan 6;9:1069543. doi: 10.3389/fsurg.2022.1069543. eCollection 2022. Front Surg. 2023. PMID: 36684151 Free PMC article. Review.
Cited by
-
An open-source framework for pulmonary fissure completeness assessment.Comput Med Imaging Graph. 2020 Jul;83:101712. doi: 10.1016/j.compmedimag.2020.101712. Epub 2020 Feb 21. Comput Med Imaging Graph. 2020. PMID: 32115275 Free PMC article.
-
Loss of Pulmonary Vascular Volume as a Predictor of Right Ventricular Dysfunction and Mortality in Acute Pulmonary Embolism.Circ Cardiovasc Imaging. 2021 Sep;14(9):e012347. doi: 10.1161/CIRCIMAGING.120.012347. Epub 2021 Sep 21. Circ Cardiovasc Imaging. 2021. PMID: 34544259 Free PMC article.
-
Pulmonary lobe separation in expiration chest CT scans based on subject-specific priors derived from inspiration scans.J Med Imaging (Bellingham). 2018 Jan;5(1):014003. doi: 10.1117/1.JMI.5.1.014003. Epub 2018 Feb 9. J Med Imaging (Bellingham). 2018. PMID: 29487878 Free PMC article.
-
Pulmonary Fissure Segmentation in CT Images Using Image Filtering and Machine Learning.Tomography. 2024 Oct 9;10(10):1645-1664. doi: 10.3390/tomography10100121. Tomography. 2024. PMID: 39453038 Free PMC article.
-
Quantification of Arterial and Venous Morphologic Markers in Pulmonary Arterial Hypertension Using CT Imaging.Chest. 2021 Dec;160(6):2220-2231. doi: 10.1016/j.chest.2021.06.069. Epub 2021 Jul 13. Chest. 2021. PMID: 34270966 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
- R01 HL089897/HL/NHLBI NIH HHS/United States
- 2R01HL089897-06A1/HL/NHLBI NIH HHS/United States
- R01HL116473/HL/NHLBI NIH HHS/United States
- U01 HL089897/HL/NHLBI NIH HHS/United States
- R01 HL116931/HL/NHLBI NIH HHS/United States
- R01 HL116473/HL/NHLBI NIH HHS/United States
- 1R01HL116931-01/HL/NHLBI NIH HHS/United States
- 1P50HL107192/HL/NHLBI NIH HHS/United States
- 2R01HL089856-06A1/HL/NHLBI NIH HHS/United States
- P50 HL107192/HL/NHLBI NIH HHS/United States
- K23HL089353-05/HL/NHLBI NIH HHS/United States
- R01 HL089856/HL/NHLBI NIH HHS/United States
- K01 HL118714/HL/NHLBI NIH HHS/United States
- R01HL107246/HL/NHLBI NIH HHS/United States
- U01 HL089856/HL/NHLBI NIH HHS/United States
- K23 HL089353/HL/NHLBI NIH HHS/United States
- R01 HL107246/HL/NHLBI NIH HHS/United States
- K25 HL104085/HL/NHLBI NIH HHS/United States
- K25 HL104085-04/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
