

Preconditioning for traumatic brain injury
- PMID: 24323189
- PMCID: PMC4967531
- DOI: 10.1007/s12975-012-0226-1
Preconditioning for traumatic brain injury
Abstract
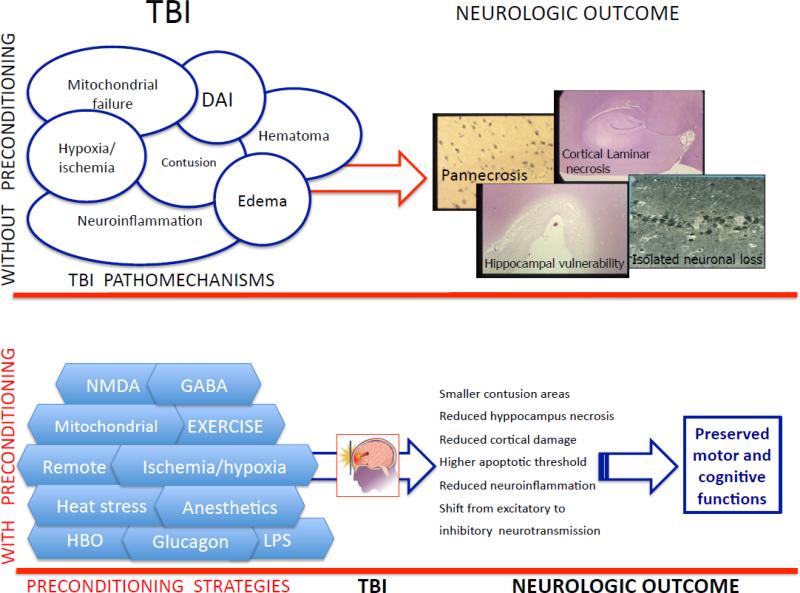
Traumatic brain injury (TBI) treatment is now focused on the prevention of primary injury and reduction of secondary injury. However, no single effective treatment is available as yet for the mitigation of traumatic brain damage in humans. Both chemical and environmental stresses applied before injury have been shown to induce consequent protection against post-TBI neuronal death. This concept termed "preconditioning" is achieved by exposure to different pre-injury stressors to achieve the induction of "tolerance" to the effect of the TBI. However, the precise mechanisms underlying this "tolerance" phenomenon are not fully understood in TBI, and therefore even less information is available about possible indications in clinical TBI patients. In this review, we will summarize TBI pathophysiology, and discuss existing animal studies demonstrating the efficacy of preconditioning in diffuse and focal type of TBI. We will also review other non-TBI preconditioning studies, including ischemic, environmental, and chemical preconditioning, which maybe relevant to TBI. To date, no clinical studies exist in this field, and we speculate on possible future clinical situations, in which pre-TBI preconditioning could be considered.
Figures
References
-
- Langlois JA, Marr A, Mitchko J, Johnson RL. Tracking the silent epidemic and educating the public: CDC's traumatic brain injury-associated activities under the TBI Act of 1996 and the Children's Health Act of 2000. J Head Trauma Rehabil. 2005;20(3):196–204. - PubMed
-
- Binder S, Corrigan JD, Langlois JA. The public health approach to traumatic brain injury: an overview of CDC's research and programs. J Head Trauma Rehabil. 2005;20(3):189–95. - PubMed
-
- Fu ES, Tummala RP. Neuroprotection in brain and spinal cord trauma. Curr Opin Anaesthesiol. 2005;18(2):181–7. doi:10.1097/01.aco.0000162838.56344.88. - PubMed
-
- Cole TB. Global road safety crisis remedy sought: 1.2 million killed, 50 million injured annually. JAMA. 2004;291(21):2531–2. doi:10.1001/jama.291.21.2531. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
