

Radiolucent lesions of the mandible: a pattern-based approach to diagnosis
- PMID: 24323536
- PMCID: PMC3948901
- DOI: 10.1007/s13244-013-0298-9
Radiolucent lesions of the mandible: a pattern-based approach to diagnosis
Abstract
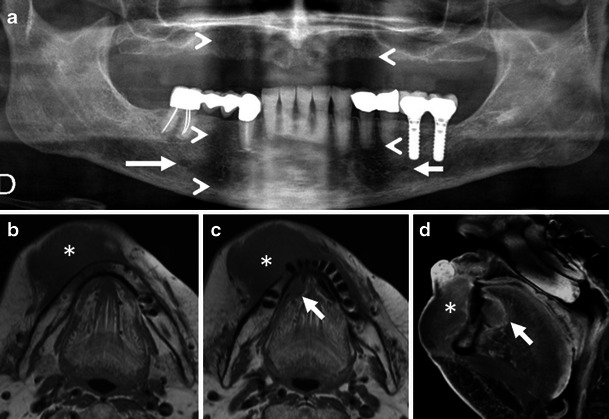
Objectives: Radiolucent mandibular lesions seen on panoramic radiographs develop from both odontogenic and non-odontogenic structures. They represent a broad spectrum of lesions with a varying degree of malignant potential. The purpose of this review is to illustrate the characteristic imaging findings-as well as the clinical and histological features-of common and uncommon radiolucent lesions of the mandible.
Methods: This review article is based on the retrospective evaluation of 11,725 panoramic radiographs seen in our institution during the past 6 years. It provides a comprehensive, practical approach to the radiological interpretation of radiolucent lesions of the mandible. To facilitate the diagnostic approach, we have classified radiolucent lesions into two groups: lesions with well-defined borders and those with ill-defined borders.
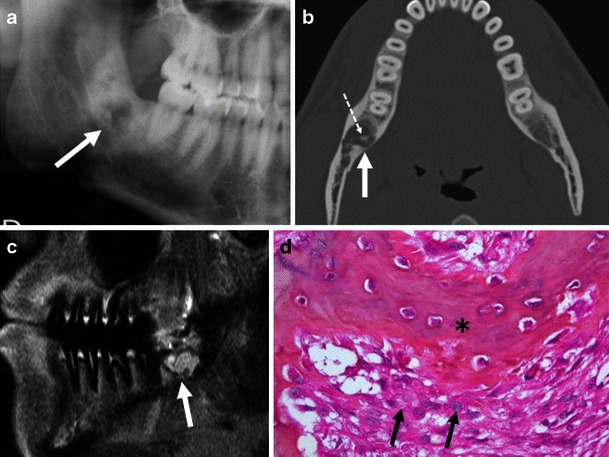
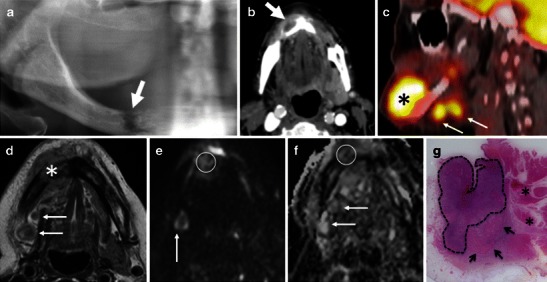
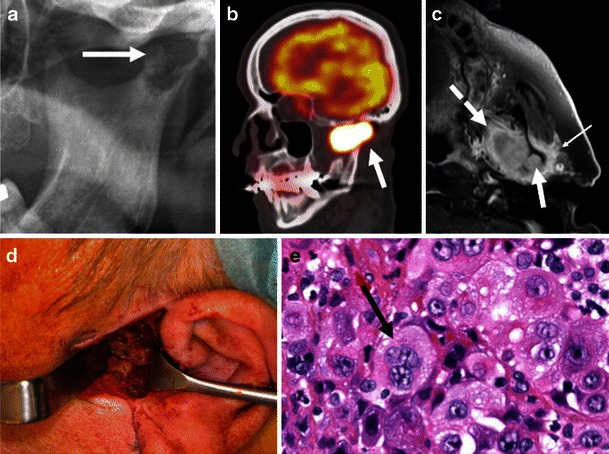
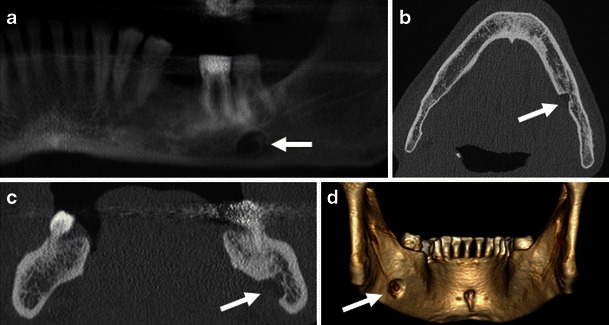
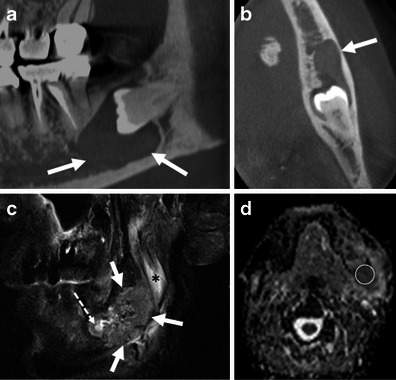
Results: Lesion prevalence, age of manifestation, location within the mandible, relationship to dental structures, effect on adjacent structures and characteristic findings at computed tomography (CT), cone beam CT (CBCT) and magnetic resonance imaging (MRI) with diffusion-weighted imaging (DWI) are discussed. Pitfalls including malignant lesions mimicking benign disease and pseudo-lesions are equally addressed.
Conclusion: Knowledge of the characteristic imaging features of radiolucent mandibular lesions narrows the differential diagnosis and is crucial for the identification of those lesions, where biopsy is indicated for definitive histology.
Teaching points: • Panoramic X-rays, CT and MRI are essential for the work-up of radiolucent mandibular lesions. • Lesion borders, location within the mandible, relationship to dental structures and tissue characteristics on cross-sectional imaging are indispensable to narrow the differential diagnosis. • High-resolution CT and CBCT play a major role for the assessment of lesion margins and their relationship to important anatomic structures, such as the inferior alveolar nerve. • Although most radiolucent lesions with well-defined sclerotic borders are benign, MRI may reveal clinically unsuspected malignant disease.
Figures
References
-
- Cotti E, Campisi G. Advanced radiographic techniques for the detection of lesions in bone. Endod Top. 2004;7:52–72. doi: 10.1111/j.1601-1546.2004.00064.x. - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
