

Outcome-driven thresholds for ambulatory pulse pressure in 9938 participants recruited from 11 populations
- PMID: 24324050
- PMCID: PMC3998649
- DOI: 10.1161/HYPERTENSIONAHA.113.02179
Outcome-driven thresholds for ambulatory pulse pressure in 9938 participants recruited from 11 populations
Erratum in
- Hypertension. 2014 May;63(5):e128
Abstract
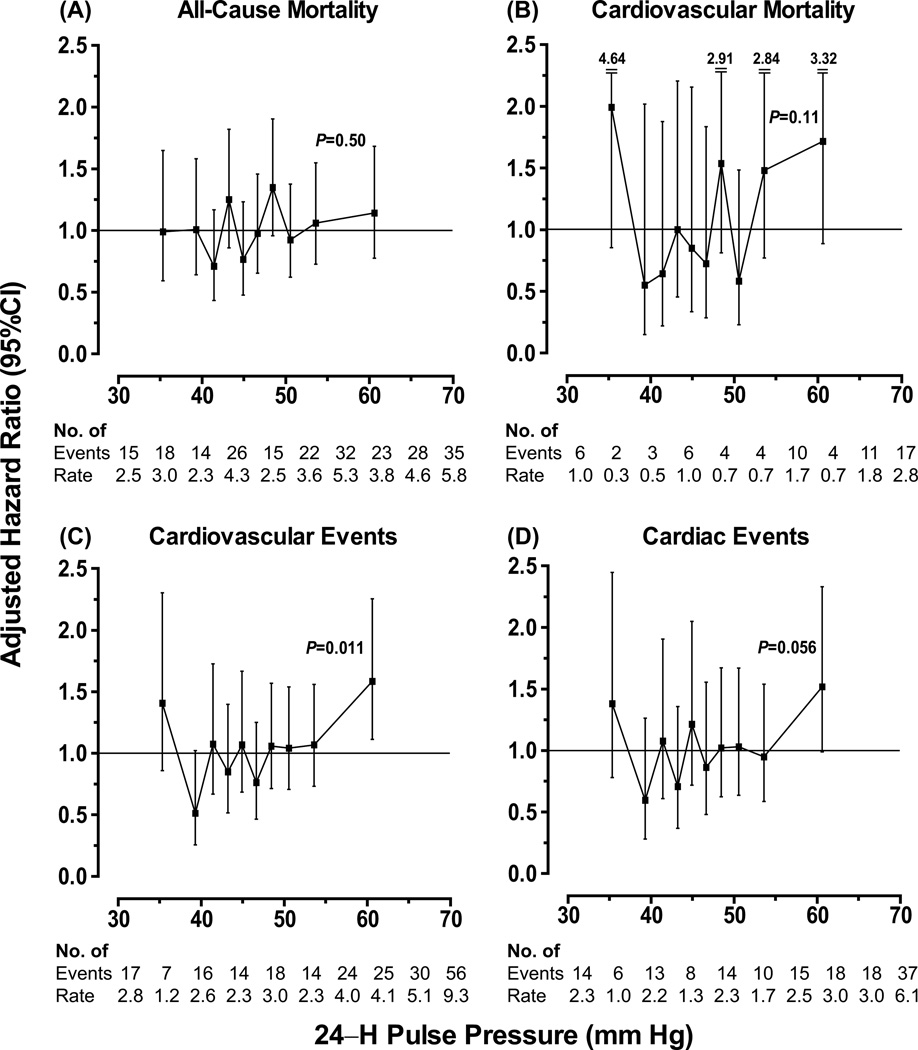
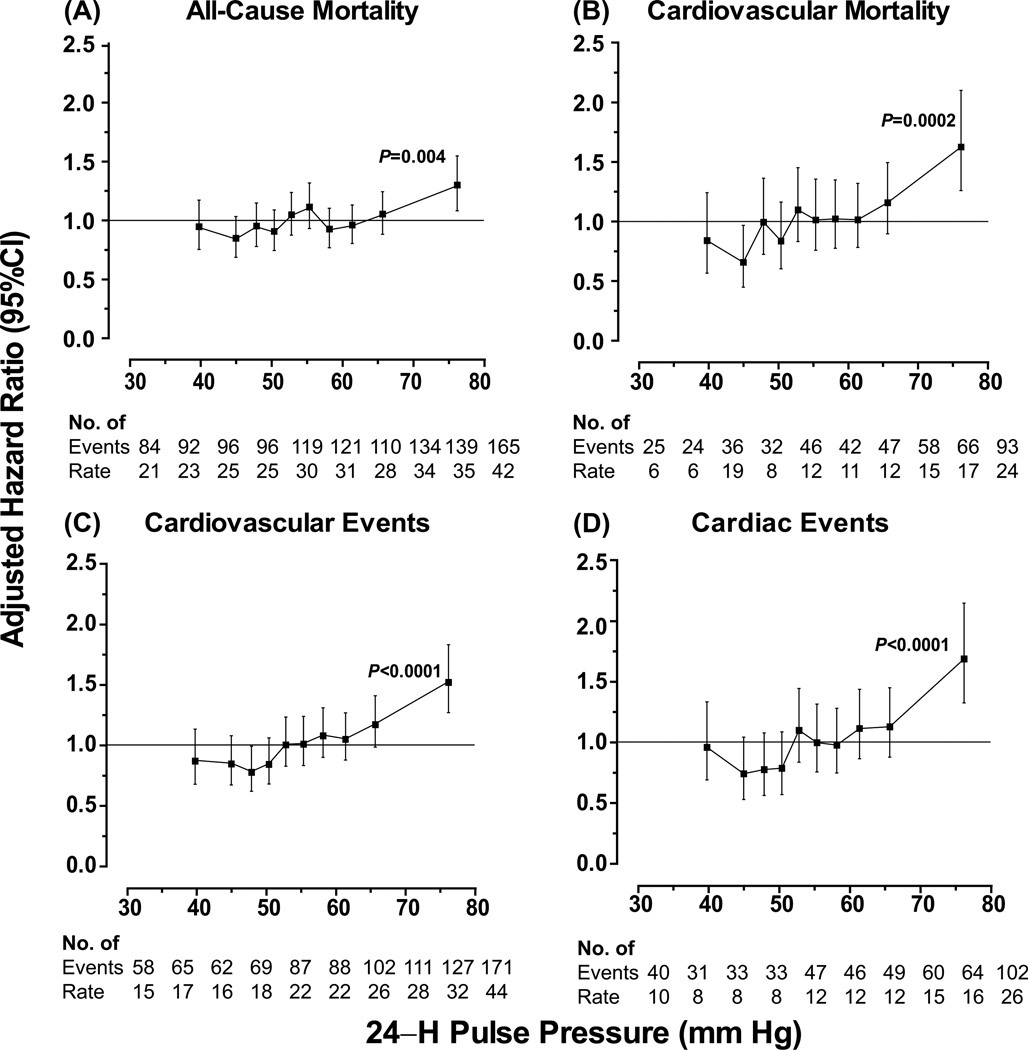
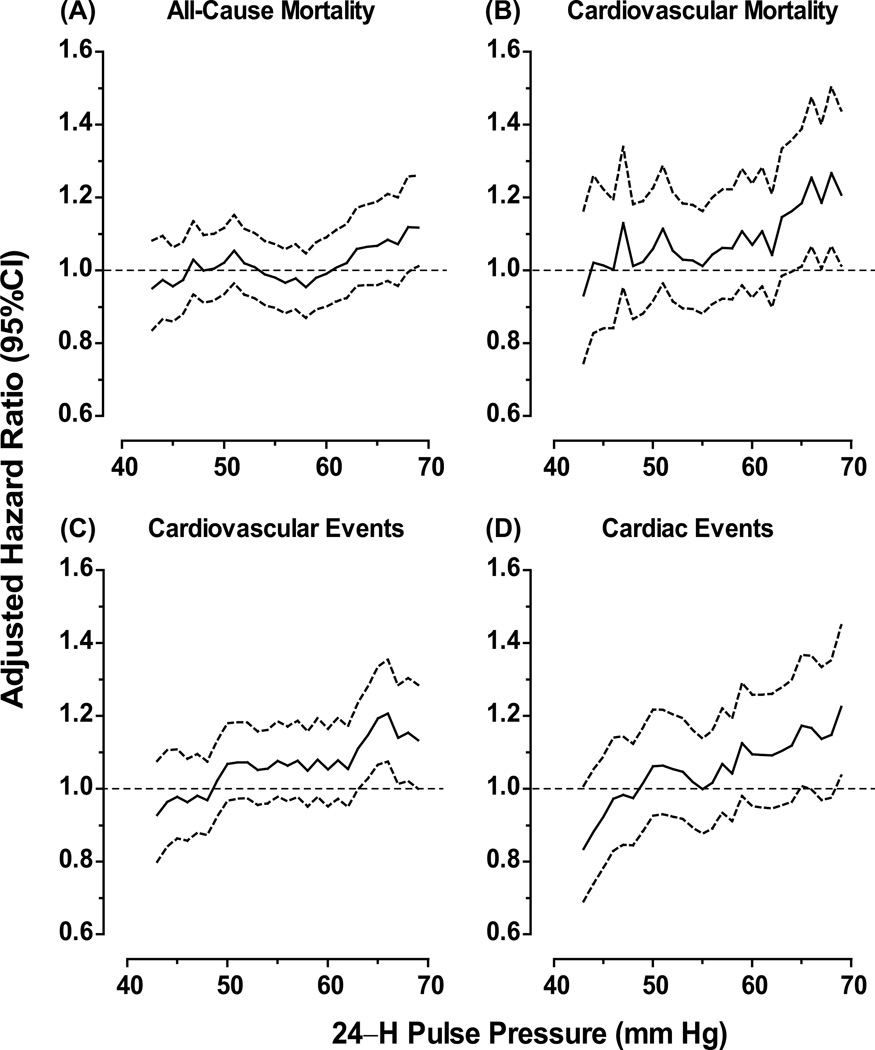
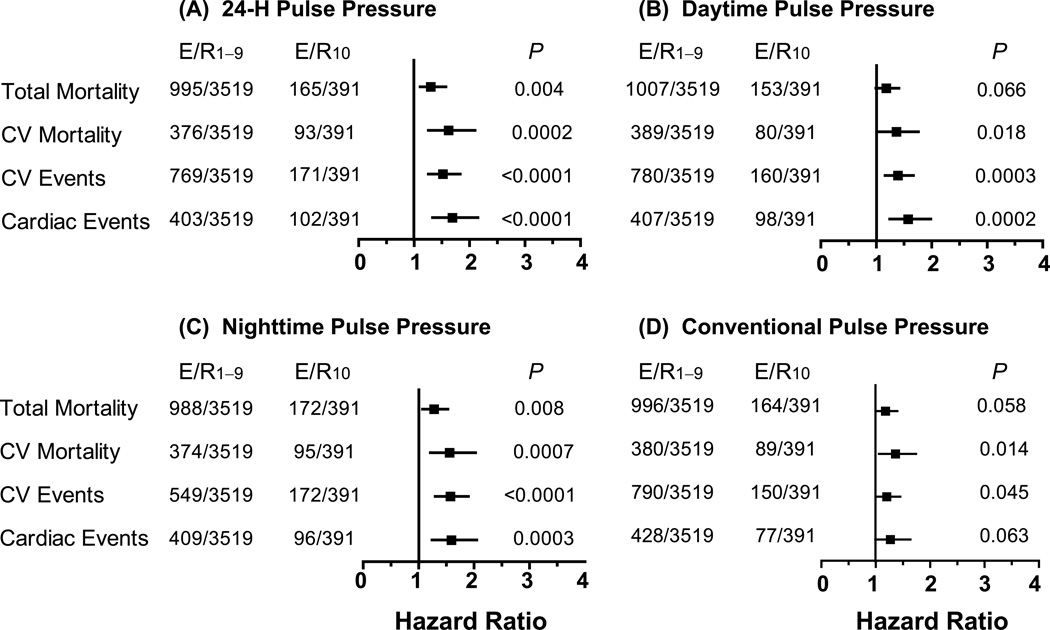
Evidence-based thresholds for risk stratification based on pulse pressure (PP) are currently unavailable. To derive outcome-driven thresholds for the 24-hour ambulatory PP, we analyzed 9938 participants randomly recruited from 11 populations (47.3% women). After age stratification (<60 versus ≥60 years) and using average risk as reference, we computed multivariable-adjusted hazard ratios (HRs) to assess risk by tenths of the PP distribution or risk associated with stepwise increasing (+1 mm Hg) PP levels. All adjustments included mean arterial pressure. Among 6028 younger participants (68 853 person-years), the risk of cardiovascular (HR, 1.58; P=0.011) or cardiac (HR, 1.52; P=0.056) events increased only in the top PP tenth (mean, 60.6 mm Hg). Using stepwise increasing PP levels, the lower boundary of the 95% confidence interval of the successive thresholds did not cross unity. Among 3910 older participants (39 923 person-years), risk increased (P≤0.028) in the top PP tenth (mean, 76.1 mm Hg). HRs were 1.30 and 1.62 for total and cardiovascular mortality, and 1.52, 1.69, and 1.40 for all cardiovascular, cardiac, and cerebrovascular events. The lower boundary of the 95% confidence interval of the HRs associated with stepwise increasing PP levels crossed unity at 64 mm Hg. While accounting for all covariables, the top tenth of PP contributed less than 0.3% (generalized R(2) statistic) to the overall risk among the elderly. Thus, in randomly recruited people, ambulatory PP does not add to risk stratification below age 60; in the elderly, PP is a weak risk factor with levels below 64 mm Hg probably being innocuous.
Keywords: ambulatory blood pressure; epidemiology; population science; pulse pressure.
Figures
Comment in
-
Ambulatory pulse pressure: does it improve cardiovascular risk stratification?Hypertension. 2014 Feb;63(2):217-9. doi: 10.1161/HYPERTENSIONAHA.113.02436. Epub 2013 Dec 9. Hypertension. 2014. PMID: 24324036 No abstract available.
References
-
- Safar ME, Levy BI, Struijker-Boudier H. Current perspectives on arterial stiffness and pulse pressure in hypertension and cardiovascular diseases. Circulation. 2003;107:2864–2869. - PubMed
-
- Staessen J, Amery A, Fagard R. Editorial review. Isolated systolic hypertension. J Hypertens. 1990;8:393–405. - PubMed
-
- Franklin SS, Larson MG, Khan SA, Wong ND, Leip EP, Kannel WB, Levy D. Does the relation of blood pressure to coronary heart disease change with aging? The Framingham Heart Study. Circulation. 2001;103:1245–1249. - PubMed
-
- Bangalore S, Messerli FH, Franklin SS, Mancia G, Champion A, Pepine CJ. Pulse pressure and risk of cardiovascular outcomes in patients with hypertension and coronary artery disease: an INternational VErapamil SR-trandolapril STudy (INVEST) analysis. Eur Heart J. 2009;30:1395–1401. - PubMed
-
- Amar J, Vernier I, Rossignol E, Bongard V, Arnaud C, Conte JJ, Salvador M, Chamontin B. Nocturnal blood pressure and 24-hour pulse pressure are potent indicators of mortality in hemodialysis patients. Kidney Intern. 2000;57:2485–2491. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
