

Efficacy of abatacept for arthritis in patients with an overlap syndrome between rheumatoid arthritis and systemic lupus erythematosus
- PMID: 24324510
- PMCID: PMC3845485
- DOI: 10.1155/2013/697525
Efficacy of abatacept for arthritis in patients with an overlap syndrome between rheumatoid arthritis and systemic lupus erythematosus
Abstract
Introduction: This study aimed to investigate the efficacy of abatacept for arthritis in patients with rhupus, an overlap syndrome between rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE).
Methods: Patients who fulfilled both the 2010 ACR/EULAR criteria for RA classification and the 1997 ACR revised criteria for classification of SLE and received abatacept treatment for arthritis were retrospectively studied.
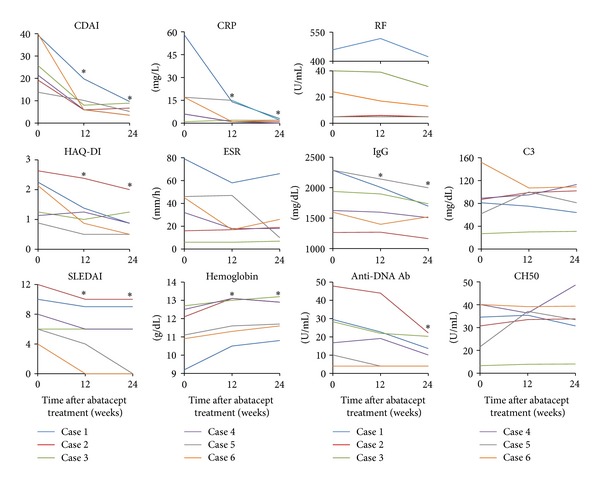
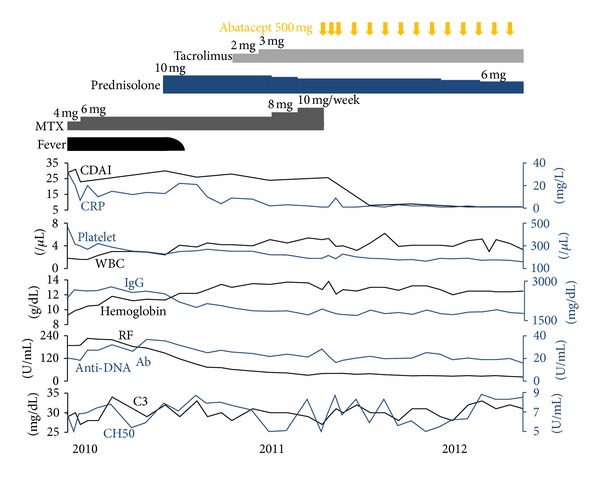
Results: Six rhupus patients who fulfilled the inclusion criteria above were identified. All patients had active arthritis despite receiving antirheumatic drugs including methotrexate when abatacept was initiated. Clinical Disease Activity Index (CDAI) significantly decreased between baseline and 12 weeks (P = 0.028) and remained low through 24 weeks. All patients achieved either a good or moderate response according to the EULAR response criteria at 24 weeks. Health Assessment Questionnaire-Disability Index (HAQ-DI) also significantly decreased between baseline and 24 weeks (P = 0.043). In addition, the levels of immunoglobulin G and anti-DNA antibody significantly decreased between baseline and 24 weeks (P = 0.028 and P = 0.043, resp.).
Conclusions: Treatment with abatacept is likely to be efficacious in patients with rhupus whose arthritis is refractory to methotrexate. In addition, abatacept may have a moderate effect on abnormal antibody production in rhupus patients.
Figures
Similar articles
-
Real-world effectiveness of abatacept for rheumatoid arthritis treatment in European and Canadian populations: a 6-month interim analysis of the 2-year, observational, prospective ACTION study.BMC Musculoskelet Disord. 2014 Jan 11;15:14. doi: 10.1186/1471-2474-15-14. BMC Musculoskelet Disord. 2014. PMID: 24410774 Free PMC article.
-
Efficacy and safety of the selective co-stimulation modulator abatacept following 2 years of treatment in patients with rheumatoid arthritis and an inadequate response to anti-tumour necrosis factor therapy.Ann Rheum Dis. 2008 Apr;67(4):547-54. doi: 10.1136/ard.2007.074773. Epub 2007 Oct 5. Ann Rheum Dis. 2008. PMID: 17921185 Clinical Trial.
-
Decreased external home help use with improved clinical status in rheumatoid arthritis: an exploratory analysis of the Abatacept in Inadequate responders to Methotrexate (AIM) trial.Clin Ther. 2008 Apr;30(4):734-48. doi: 10.1016/j.clinthera.2008.03.015. Clin Ther. 2008. PMID: 18498922 Clinical Trial.
-
Indirect treatment comparison of abatacept with methotrexate versus other biologic agents for active rheumatoid arthritis despite methotrexate therapy in the United kingdom.J Rheumatol. 2012 Jun;39(6):1198-206. doi: 10.3899/jrheum.111345. Epub 2012 Apr 15. J Rheumatol. 2012. PMID: 22505698 Review.
-
How to treat refractory arthritis in lupus?Joint Bone Spine. 2012 Jul;79(4):347-50. doi: 10.1016/j.jbspin.2011.12.010. Epub 2012 Feb 14. Joint Bone Spine. 2012. PMID: 22341583 Review.
Cited by
-
Long-term efficacy and safety of antitumour necrosis factor alpha treatment in rhupus: an open-label study of 15 patients.RMD Open. 2017 Dec 29;3(2):e000555. doi: 10.1136/rmdopen-2017-000555. eCollection 2017. RMD Open. 2017. PMID: 29435362 Free PMC article.
-
Rhupus; unusual presentations.Clin Rheumatol. 2015 Dec;34(12):2041-6. doi: 10.1007/s10067-015-2978-y. Epub 2015 May 28. Clin Rheumatol. 2015. PMID: 26017231
-
Ultrasonographic assessment of bone erosions in the different subtypes of systemic lupus erythematosus arthritis: comparison with computed tomography.Arthritis Res Ther. 2016 Oct 4;18(1):222. doi: 10.1186/s13075-016-1125-8. Arthritis Res Ther. 2016. PMID: 27716316 Free PMC article.
-
Need for Greater Attention to Joint Damage in Rhupus Patients: Results from an Ultrasound Study.Med Sci Monit. 2020 Oct 28;26:e927104. doi: 10.12659/MSM.927104. Med Sci Monit. 2020. PMID: 33112843 Free PMC article.
-
Examining the clinical and radiological landscape of rhupus: navigating the challenges in disease classification.Rheumatol Int. 2024 Jul;44(7):1185-1196. doi: 10.1007/s00296-024-05561-0. Epub 2024 Mar 21. Rheumatol Int. 2024. PMID: 38512479 Review.
References
-
- Panush RS, Edwards L, Longley S, Webster E. ‘Rhupus’ syndrome. Archives of Internal Medicine. 1988;148(7):1633–1636. - PubMed
-
- Chan MT, Owen P, Dunphy J, et al. Associations of erosive arthritis with anti-cyclic citrullinated peptide antibodies and MHC class II alleles in systemic lupus erythematosus. Journal of Rheumatology. 2008;35(1):77–83. - PubMed
-
- Ball EM, Bell AL. Lupus arthritis-do we have a clinically useful classification? Rheumatology. 2012;51(5):771–779.ker381 - PubMed
-
- Gabba A, Piga M, Vacca A, et al. Joint and tendon involvement in systemic lupus erythematosus: an ultrasound study of hands and wrists in 108 patients. Rheumatology. 2012;51(12):2278–2285. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical