

Whole genome sequencing reveals complex evolution patterns of multidrug-resistant Mycobacterium tuberculosis Beijing strains in patients
- PMID: 24324807
- PMCID: PMC3855793
- DOI: 10.1371/journal.pone.0082551
Whole genome sequencing reveals complex evolution patterns of multidrug-resistant Mycobacterium tuberculosis Beijing strains in patients
Abstract
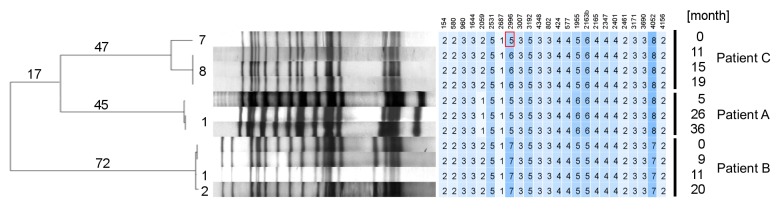
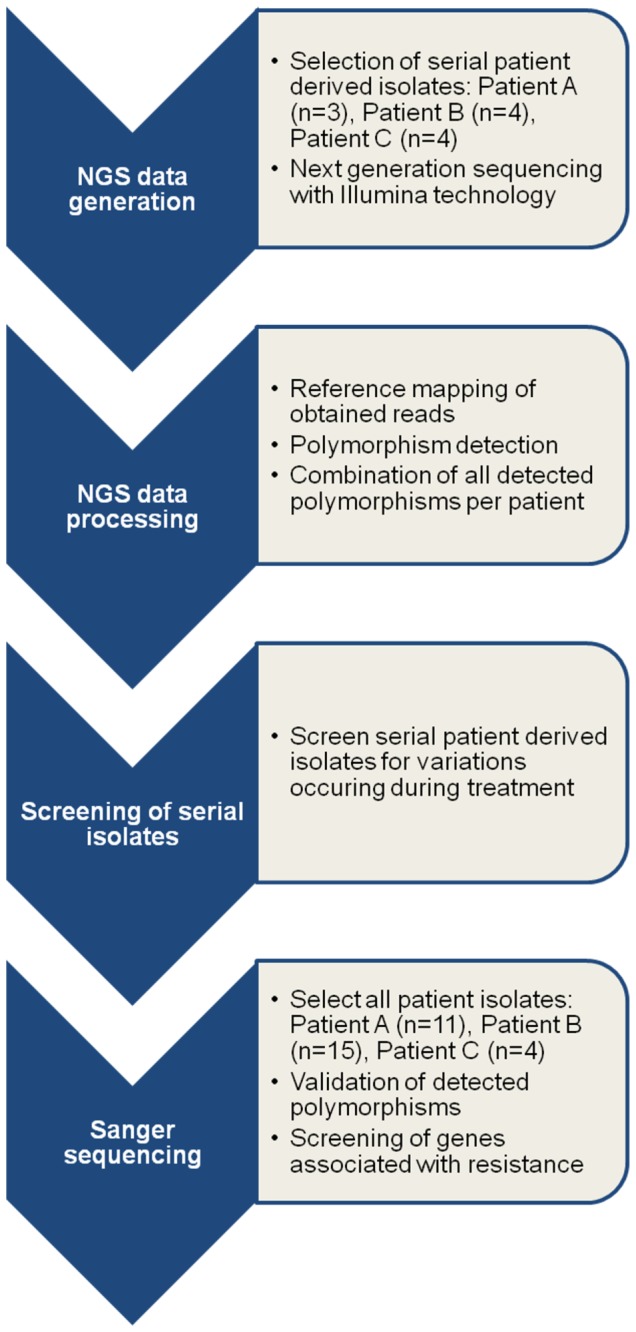
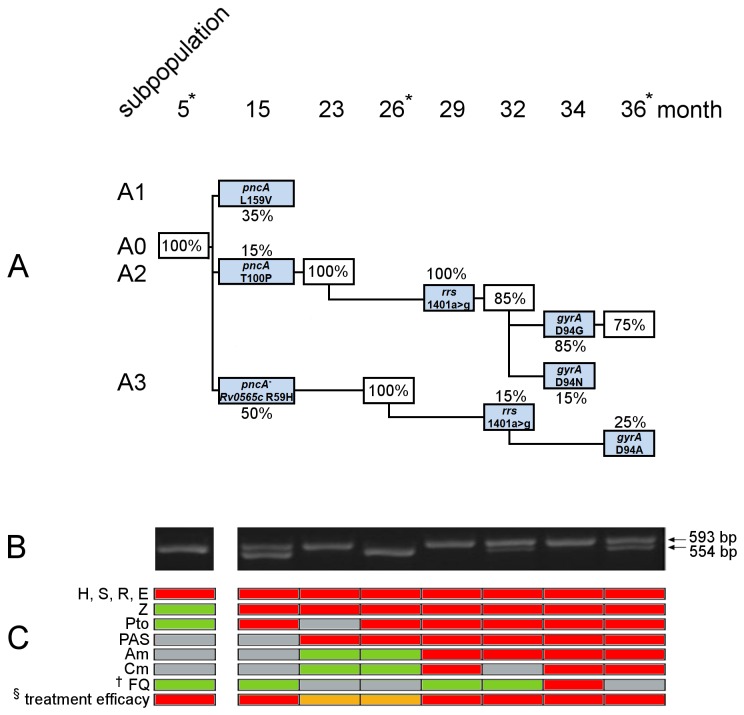
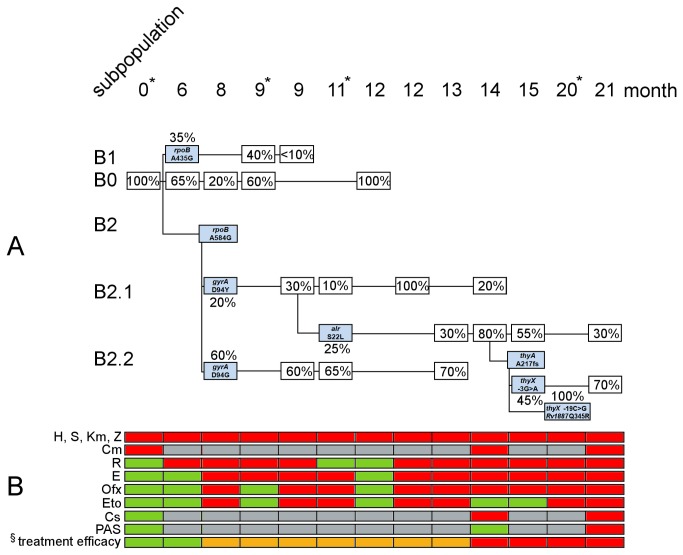
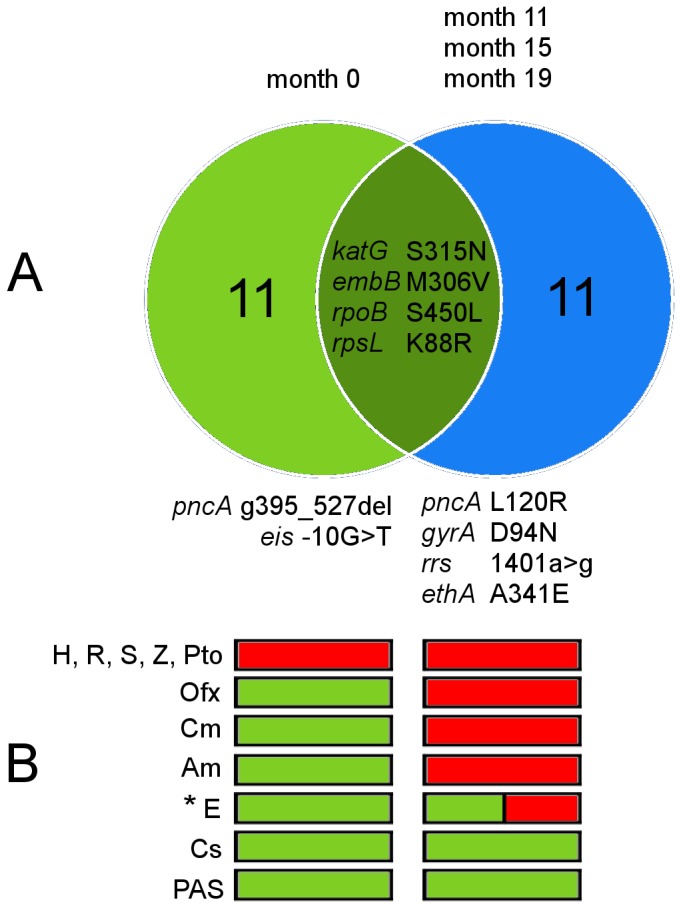
Multidrug-resistant (MDR) Mycobacterium tuberculosis complex (MTBC) strains represent a major threat for tuberculosis (TB) control. Treatment of MDR-TB patients is long and less effective, resulting in a significant number of treatment failures. The development of further resistances leads to extensively drug-resistant (XDR) variants. However, data on the individual reasons for treatment failure, e.g. an induced mutational burst, and on the evolution of bacteria in the patient are only sparsely available. To address this question, we investigated the intra-patient evolution of serial MTBC isolates obtained from three MDR-TB patients undergoing longitudinal treatment, finally leading to XDR-TB. Sequential isolates displayed identical IS6110 fingerprint patterns, suggesting the absence of exogenous re-infection. We utilized whole genome sequencing (WGS) to screen for variations in three isolates from Patient A and four isolates from Patient B and C, respectively. Acquired polymorphisms were subsequently validated in up to 15 serial isolates by Sanger sequencing. We determined eight (Patient A) and nine (Patient B) polymorphisms, which occurred in a stepwise manner during the course of the therapy and were linked to resistance or a potential compensatory mechanism. For both patients, our analysis revealed the long-term co-existence of clonal subpopulations that displayed different drug resistance allele combinations. Out of these, the most resistant clone was fixed in the population. In contrast, baseline and follow-up isolates of Patient C were distinguished each by eleven unique polymorphisms, indicating an exogenous re-infection with an XDR strain not detected by IS6110 RFLP typing. Our study demonstrates that intra-patient microevolution of MDR-MTBC strains under longitudinal treatment is more complex than previously anticipated. However, a mutator phenotype was not detected. The presence of different subpopulations might confound phenotypic and molecular drug resistance tests. Furthermore, high resolution WGS analysis is necessary to accurately detect exogenous re-infection as classical genotyping lacks discriminatory power in high incidence settings.
Conflict of interest statement
Figures
References
-
- WHO (2012) WHO | Tuberculosis Fact sheet. WHO. Available: http://www.who.int/mediacentre/factsheets/fs104/en/. Accessed 5 April 2012
-
- Ahuja SD, Ashkin D, Avendano M, Banerjee R, Bauer M et al. (2012) Multidrug resistant pulmonary tuberculosis treatment regimens and patient outcomes: an individual patient data meta-analysis of 9,153 patients. PLoS Med 9: e1001300. doi: 10.1371/journal.pmed.1001300. PubMed: 22952439. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
