

Multimodality monitoring in the neurointensive care unit: a special perspective for patients with stroke
- PMID: 24324945
- PMCID: PMC3779668
- DOI: 10.5853/jos.2013.15.2.99
Multimodality monitoring in the neurointensive care unit: a special perspective for patients with stroke
Abstract
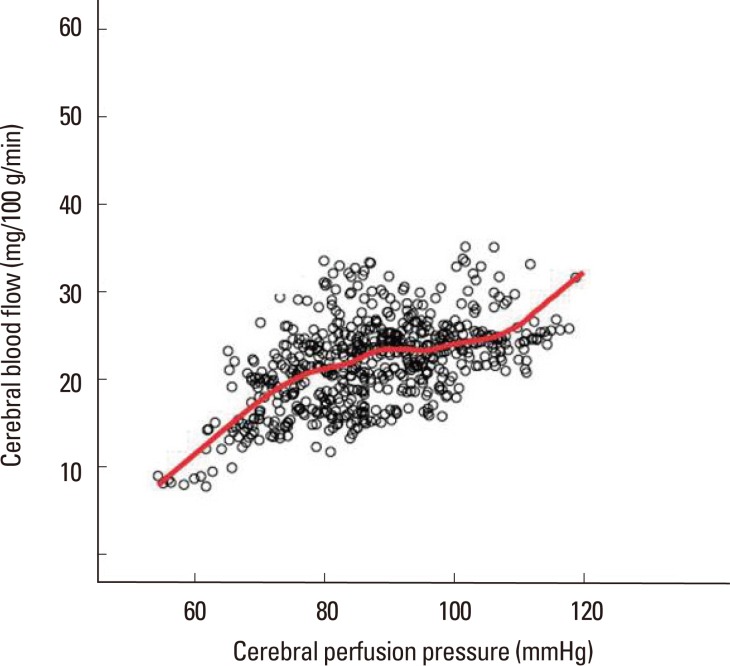
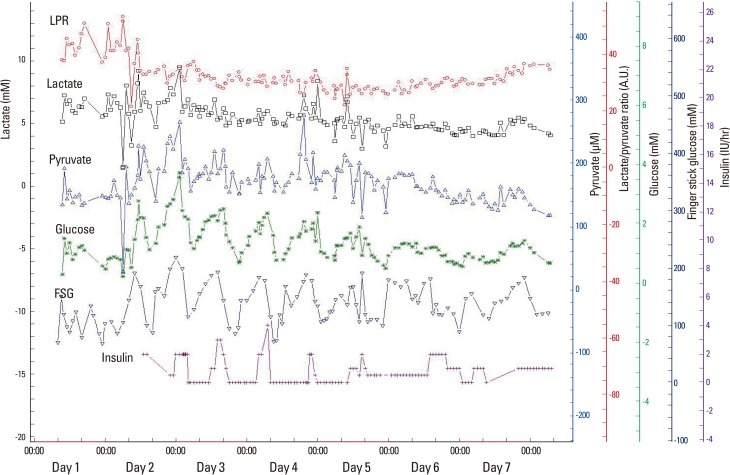
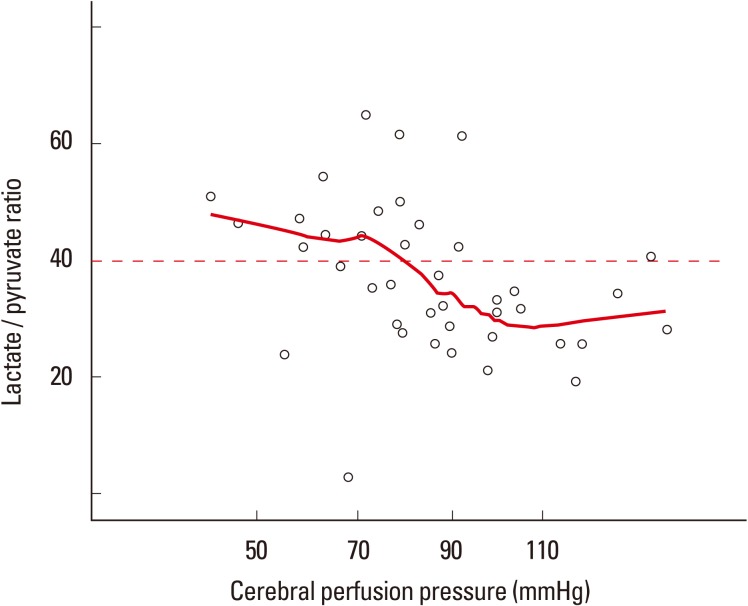
Multimodality monitoring (MMM) is a recently developed method that aids in understanding real-time brain physiology. Early detection of physiological disturbances is possible with the help of MMM, which allows identification of underlying causes of deterioration and minimization of secondary brain injury (SBI). MMM is especially helpful in comatose patients with severe brain injury because neurological examinations are not sensitive enough to detect SBI. The variables frequently examined in MMM are hemodynamic parameters such as intracranial pressure, cerebral perfusion pressure, and mean arterial pressure; brainspecific oxygen tension; markers for brain metabolism including glucose, lactate, and pyruvate levels in brain tissue; and cerebral blood flow. Continuous electroencephalography can be performed, if needed. The majority of SBIs stem from brain tissue hypoxia, brain ischemia, and seizures, which lead to a disturbance in brain oxygen levels, cerebral blood flow, and electrical discharges, all of which are easily detected by MMM. In this review, we discuss the clinical importance of physiological variables as well as the practical applicability of MMM in patients with stroke.
Keywords: Coma; Critical care; Physiologic monitoring; Stroke.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Kramer AH, Zygun DA. Do neurocritical care units save lives? Measuring the impact of specialized ICUs. Neurocrit Care. 2011;14:329–333. - PubMed
-
- Wright WL. Multimodal monitoring in the ICU: when could it be useful? J Neurol Sci. 2007;261:10–15. - PubMed
-
- Sahuquillo J. Does multimodality monitoring make a difference in neurocritical care? Eur J Anaesthesiol Suppl. 2008;42:83–86. - PubMed
-
- Hemphill JC, Andrews P, De Georgia M. Multimodal monitoring and neurocritical care bioinformatics. Nat Rev Neurol. 2011;7:451–460. - PubMed
-
- Le Roux P. Physiological monitoring of the severe traumatic brain injury patient in the intensive care unit. Curr Neurol Neurosci Rep. 2013;13:331. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
