

Impact of forced vital capacity loss on survival after the onset of chronic lung allograft dysfunction
- PMID: 24325429
- PMCID: PMC3983891
- DOI: 10.1164/rccm.201306-1155OC
Impact of forced vital capacity loss on survival after the onset of chronic lung allograft dysfunction
Abstract
Rationale: Emerging evidence suggests a restrictive phenotype of chronic lung allograft dysfunction (CLAD) exists; however, the optimal approach to its diagnosis and clinical significance is uncertain.
Objectives: To evaluate the hypothesis that spirometric indices more suggestive of a restrictive ventilatory defect, such as loss of FVC, identify patients with distinct clinical, radiographic, and pathologic features, including worse survival.
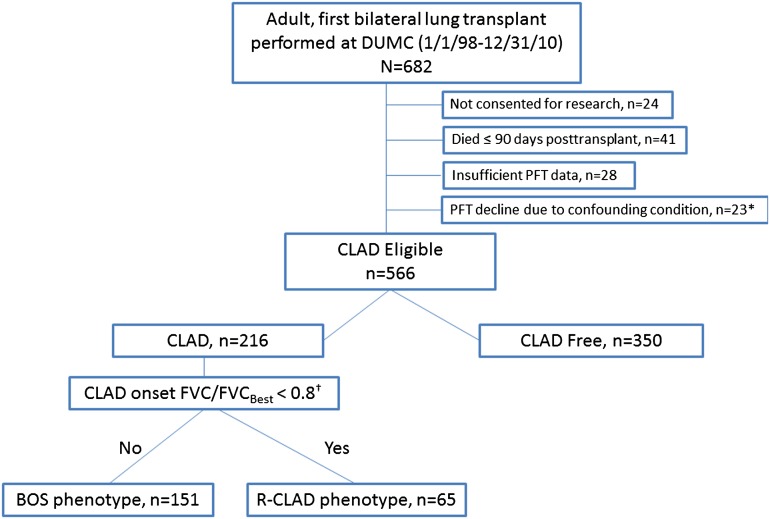
Methods: Retrospective, single-center analysis of 566 consecutive first bilateral lung recipients transplanted over a 12-year period. A total of 216 patients developed CLAD during follow-up. CLAD was categorized at its onset into discrete physiologic groups based on spirometric criteria. Imaging and histologic studies were reviewed when available. Survival after CLAD diagnosis was assessed using Kaplan-Meier and Cox proportional hazards models.
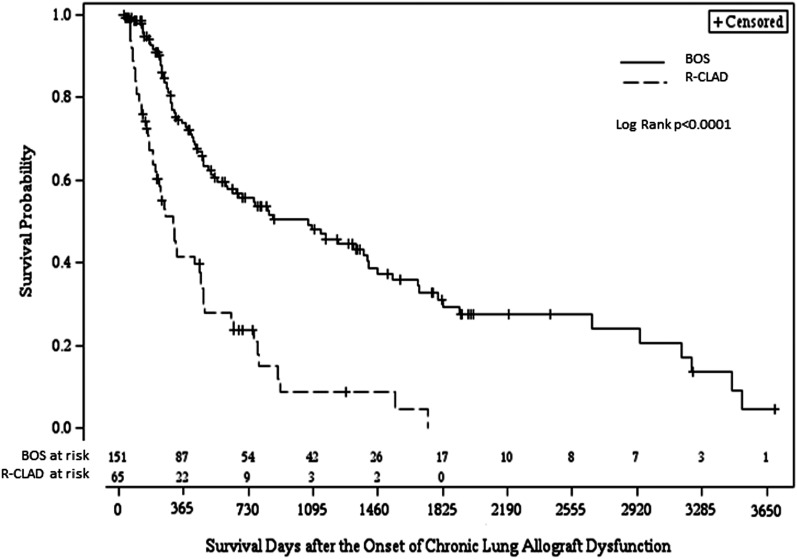
Measurements and main results: Among patients with CLAD, 30% demonstrated an FVC decrement at its onset. These patients were more likely to be female, have radiographic alveolar or interstitial changes, and histologic findings of interstitial fibrosis. Patients with FVC decline at CLAD onset had significantly worse survival after CLAD when compared with those with preserved FVC (P < 0.0001; 3-yr survival estimates 9% vs. 48%, respectively). The deleterious impact of CLAD accompanied by FVC loss on post-CLAD survival persisted in a multivariable model including baseline demographic and clinical factors (P < 0.0001; adjusted hazard ratio, 2.73; 95% confidence interval, 1.86-4.04).
Conclusions: At CLAD onset, a subset of patients demonstrating physiology more suggestive of restriction experience worse clinical outcomes. Further study of the biologic mechanisms underlying CLAD phenotypes is critical to improving long-term survival after lung transplantation.
Figures
References
-
- Christie JD, Edwards LB, Kucheryavaya AY, Benden C, Dipchand AI, Dobbels F, Kirk R, Rahmel AO, Stehlik J, Hertz MI International Society of Heart and Lung Transplantation. The Registry of the International Society for Heart and Lung Transplantation: 29th adult lung and heart-lung transplant report-2012. J Heart Lung Transplant. 2012;31:1073–1086. - PubMed
-
- Sato M. Chronic lung allograft dysfunction after lung transplantation: the moving target. Gen Thorac Cardiovasc Surg. 2013;61:67–78. - PubMed
-
- Estenne M, Maurer JR, Boehler A, Egan JJ, Frost A, Hertz M, Mallory GB, Jr, Snell GI, Yousem S. Bronchiolitis obliterans syndrome 2001: an update of the diagnostic criteria. J Heart Lung Transplant. 2002;21:297–310. - PubMed
-
- Verleden GM, Vos R, Verleden SE, De Wever W, De Vleeschauwer SI, Willems-Widyastuti A, Scheers H, Dupont LJ, Van Raemdonck DE, Vanaudenaerde BM. Survival determinants in lung transplant patients with chronic allograft dysfunction. Transplantation. 2011;92:703–708. - PubMed
-
- Sato M, Waddell TK, Wagnetz U, Roberts HC, Hwang DM, Haroon A, Wagnetz D, Chaparro C, Singer LG, Hutcheon MA, et al. Restrictive allograft syndrome (RAS): a novel form of chronic lung allograft dysfunction. J Heart Lung Transplant. 2011;30:735–742. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
