

Circulating levels of soluble MER in lupus reflect M2c activation of monocytes/macrophages, autoantibody specificities and disease activity
- PMID: 24325951
- PMCID: PMC3978923
- DOI: 10.1186/ar4407
Circulating levels of soluble MER in lupus reflect M2c activation of monocytes/macrophages, autoantibody specificities and disease activity
Abstract
Introduction: Systemic lupus erythematosus (SLE) is characterized by impaired efferocytosis and aberrant activation of innate immunity. We asked if shedding of MER receptor tyrosine kinase (MerTK) and AXL into soluble (s) ectodomains was related to immunological and clinical aspects of SLE.
Methods: Levels of sMER and sAXL in the plasma of 107 SLE patients and 45 matched controls were measured by ELISA. In 40 consecutive SLE patients, we examined potential correlations between either sMER or sAXL and plasma levels of sCD163, a marker of M2 activation. All three soluble receptors were measured in supernatants of monocytes/macrophages cultured in various immunological conditions. Membrane expression of MerTK, AXL and CD163 was assessed by flow cytometry.
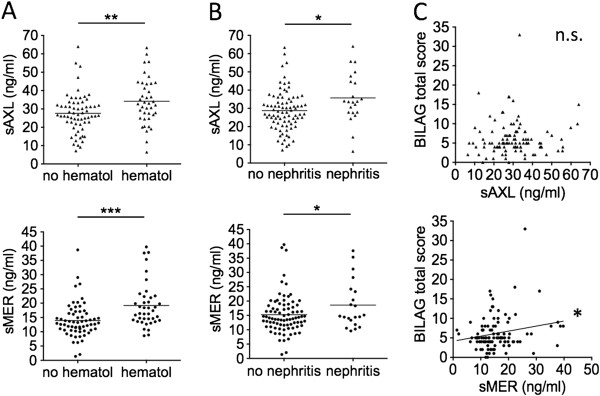
Results: Both sMER and sAXL were associated with anti-chromatin and anti-phospholipid autoantibodies, and with hematological and renal involvement. However, sMER and sAXL did not significantly correlate with each other; sAXL correlated with growth arrest-specific 6 (Gas6), whereas sMER correlated with reduced free protein S (PROS) levels. Only sMER showed significant associations with lupus-specific anti-dsDNA, anti-Sm, anti-ribonucleoprotein (anti-RNP) and anti-Ro60 autoantibodies. Strong correlations with disease activity indices (Systemic Lupus Erythematosus Disease Activity Index (SLEDAI), complement reduction, titer of circulating anti-dsDNA) were found for sMER, not for sAXL. Patients with active SLEDAI, nephritis, anti-dsDNA and anti-Ro60 positivity showed higher levels of sMER compared to controls. Levels of sMER, not sAXL, correlated with sCD163 levels, and these correlated with SLEDAI. Production of sMER and sCD163 occurred under “M2c” polarizing conditions, whereas sAXL was released upon type-I IFN exposure.
Conclusions: Alterations in homeostasis of anti-inflammatory and efferocytic “M2c” monocytes/macrophages may have a role in immunopathogenesis of SLE.
Figures






References
-
- Herrmann M, Voll RE, Zoller OM, Hagenhofer M, Ponner BB, Kalden JR. Impaired phagocytosis of apoptotic cell material by monocyte-derived macrophages from patients with systemic lupus erythematosus. Arthritis Rheum. 1998;15:1241–1250. doi: 10.1002/1529-0131(199807)41:7<1241::AID-ART15>3.0.CO;2-H. - DOI - PubMed
-
- Wu X, Molinaro C, Johnson N, Casiano CA. Secondary necrosis is a source of proteolytically modified forms of specific intracellular autoantigens: implications for systemic autoimmunity. Arthritis Rheum. 2001;15:2642–2652. doi: 10.1002/1529-0131(200111)44:11<2642::AID-ART444>3.0.CO;2-8. - DOI - PubMed
-
- Vanden Berghe T, Vanlangenakker N, Parthoens E, Deckers W, Devos M, Festjens N, Guerin CJ, Brunk UT, Declercq W, Vandenabeele P. Necroptosis, necrosis and secondary necrosis converge on similar cellular disintegration features. Cell Death Differ. 2010;15:922–930. doi: 10.1038/cdd.2009.184. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
