

Musculoskeletal and prostate effects of combined testosterone and finasteride administration in older hypogonadal men: a randomized, controlled trial
- PMID: 24326421
- PMCID: PMC4073894
- DOI: 10.1152/ajpendo.00592.2013
Musculoskeletal and prostate effects of combined testosterone and finasteride administration in older hypogonadal men: a randomized, controlled trial
Abstract
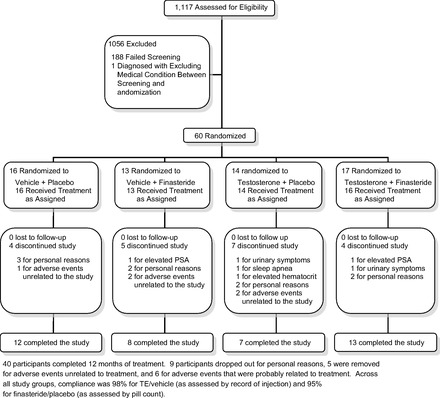
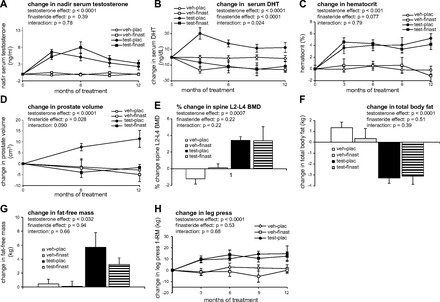
Testosterone acts directly at androgen receptors and also exerts potent actions following 5α-reduction to dihydrotestosterone (DHT). Finasteride (type II 5α-reductase inhibitor) lowers DHT and is used to treat benign prostatic hyperplasia. However, it is unknown whether elevated DHT mediates either beneficial musculoskeletal effects or prostate enlargement resulting from higher-than-replacement doses of testosterone. Our purpose was to determine whether administration of testosterone plus finasteride to older hypogonadal men could produce musculoskeletal benefits without prostate enlargement. Sixty men aged ≥60 yr with a serum testosterone concentration of ≤300 ng/dl or bioavailable testosterone ≤70 ng/dl received 52 wk of treatment with testosterone enanthate (TE; 125 mg/wk) vs. vehicle, paired with finasteride (5 mg/day) vs. placebo using a 2 × 2 factorial design. Over the course of 12 mo, TE increased upper and lower body muscle strength by 8-14% (P = 0.015 to <0.001), fat-free mass 4.04 kg (P = 0.032), lumbar spine bone mineral density (BMD) 4.19% (P < 0.001), and total hip BMD 1.96% (P = 0.024) while reducing total body fat -3.87 kg (P < 0.001) and trunk fat -1.88 kg (P = 0.0051). In the first 3 mo, testosterone increased hematocrit 4.13% (P < 0.001). Coadministration of finasteride did not alter any of these effects. Over 12 mo, testosterone also increased prostate volume 11.4 cm(3) (P = 0.0051), an effect that was completely prevented by finasteride (P = 0.0027). We conclude that a higher-than-replacement TE combined with finasteride significantly increases muscle strength and BMD and reduces body fat without causing prostate enlargement. These results demonstrate that elevated DHT mediates testosterone-induced prostate enlargement but is not required for benefits in musculoskeletal or adipose tissue.
Keywords: hypogonadal; prostate enlargement; testosterone.
Figures
References
-
- Abu EO, Horner A, Kusec V, Triffitt JT, Compston JE. The localization of androgen receptors in human bone. J Clin Endocrinol Metab 82: 3493–3497, 1997 - PubMed
-
- Amory JK, Wang C, Swerdloff RS. The effect of 5alpha-reductase inhibition with dutasteride and finasteride on semen parameters and serum hormones in healthy men. J Clin Endocrinol Metab 92: 1659–1665, 2007 - PubMed
-
- Amory JK, Watts NB, Easley KA, Sutton PR, Anawalt BD, Matsumoto AM, Bremner WJ, Tenover JL. Exogenous testosterone or testosterone with finasteride increases bone mineral density in older men with low serum testosterone. J Clin Endocrinol Metab 89: 503–510, 2004 - PubMed
-
- Barry MJ, Fowler FJ, Jr, O'Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK, Cockett AT. The American Urological Association symptom index for benign prostatic hyperplasia. The Measurement Committee of the American Urological Association. J Urol 148: 1549–1557, 1992 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical