

Pancreatic beta cell function following liraglutide-augmented weight loss in individuals with prediabetes: analysis of a randomised, placebo-controlled study
- PMID: 24326527
- PMCID: PMC5072364
- DOI: 10.1007/s00125-013-3134-3
Pancreatic beta cell function following liraglutide-augmented weight loss in individuals with prediabetes: analysis of a randomised, placebo-controlled study
Abstract
Aims/hypothesis: Liraglutide can modulate insulin secretion by directly stimulating beta cells or indirectly through weight loss and enhanced insulin sensitivity. Recently, we showed that liraglutide treatment in overweight individuals with prediabetes (impaired fasting glucose and/or impaired glucose tolerance) led to greater weight loss (-7.7% vs -3.9%) and improvement in insulin resistance compared with placebo. The current study evaluates the effects on beta cell function of weight loss augmented by liraglutide compared with weight loss alone.
Methods: This was a parallel, randomised study conducted in a single academic centre. Both participants and study administrators were blinded to treatment assignment. Individuals who were 40-70 years old, overweight (BMI 27-40 kg/m(2)) and with prediabetes were randomised (via a computerised system) to receive liraglutide (n = 35) or matching placebo (n = 33), and 49 participants were analysed. All were instructed to follow an energy-restricted diet. Primary outcome was insulin secretory function, which was evaluated in response to graded infusions of glucose and day-long mixed meals.
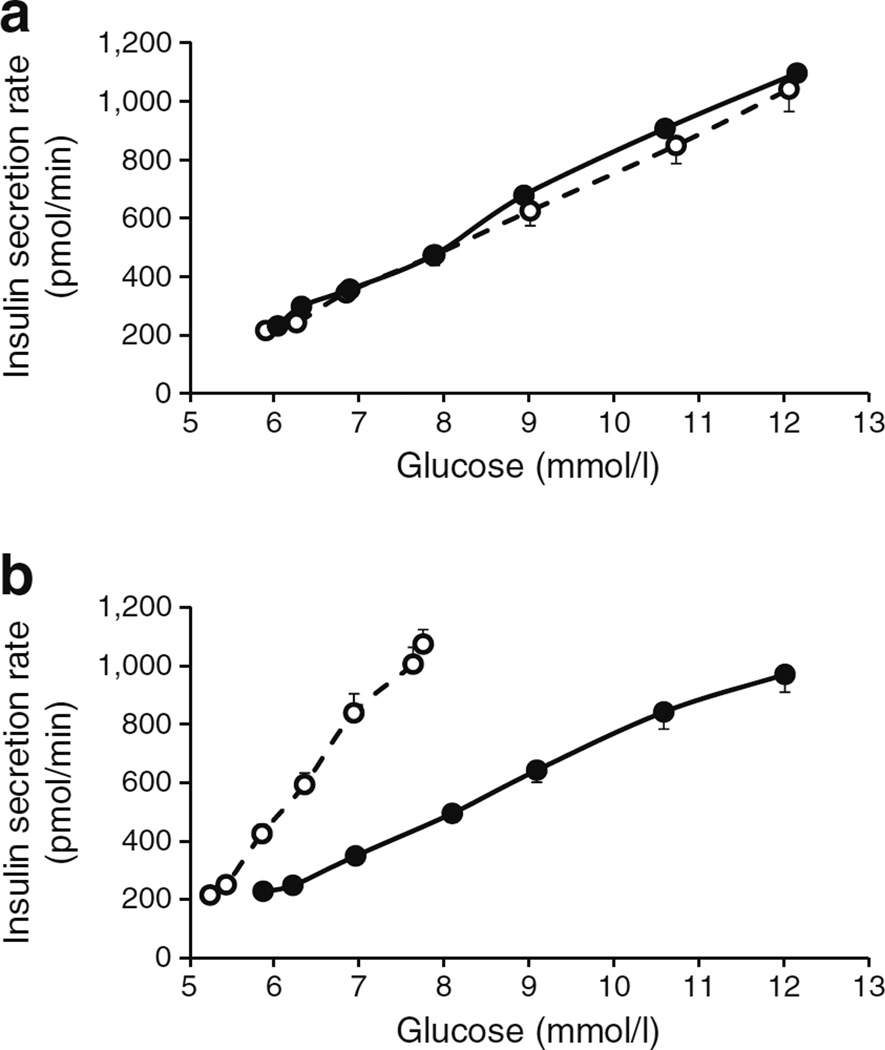
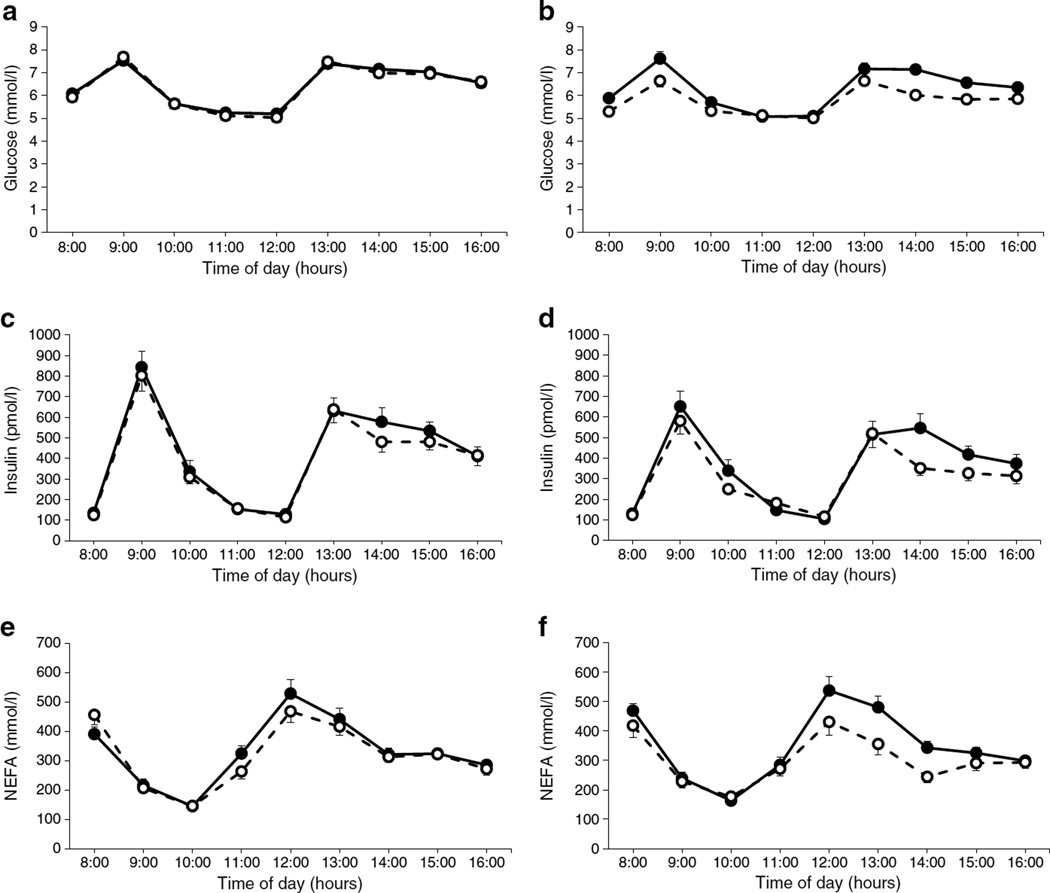
Results: Liraglutide treatment (n = 24) significantly (p ≤ 0.03) increased the insulin secretion rate (% mean change [95% CI]; 21% [12, 31] vs -4% [-11, 3]) and pancreatic beta cell sensitivity to intravenous glucose (229% [161, 276] vs -0.5% (-15, 14]), and decreased insulin clearance rate (-3.5% [-11, 4] vs 8.2 [0.2, 16]) as compared with placebo (n = 25). The liraglutide-treated group also had significantly (p ≤ 0.03) lower day-long glucose (-8.2% [-11, -6] vs -0.1 [-3, 2]) and NEFA concentrations (-14 [-20, -8] vs -2.1 [-10, 6]) following mixed meals, whereas day-long insulin concentrations did not significantly differ as compared with placebo. In a multivariate regression analysis, weight loss was associated with a decrease in insulin secretion rate and day-long glucose and insulin concentrations in the placebo group (p ≤ 0.05), but there was no association with weight loss in the liraglutide group. The most common side effect of liraglutide was nausea.
Conclusions/interpretation: A direct stimulatory effect on beta cell function was the predominant change in liraglutide-augmented weight loss. These changes appear to be independent of weight loss.
Trial registration: ClinicalTrials.gov NCT01784965 FUNDING: The study was funded by the ADA.
Figures
References
-
- Holst JJ, Deacon CF. Is there a place for incretin therapies in obesity and prediabetes? Trends Endocrinol Metab. 2013;24:145–152. - PubMed
-
- Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344:1343–1350. - PubMed
-
- Pan XR, Li GW, Hu YH, et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care. 1997;20:537–544. - PubMed
-
- Saito T, Watanabe M, Nishida J, et al. Lifestyle modification and prevention of type 2 diabetes in overweight Japanese with impaired fasting glucose levels: a randomized controlled trial. Arch Intern Med. 2011;171:1352–1360. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
