

Deltoid-split or deltopectoral approaches for the treatment of displaced proximal humeral fractures?
- PMID: 24326593
- PMCID: PMC3971224
- DOI: 10.1007/s11999-013-3415-7
Deltoid-split or deltopectoral approaches for the treatment of displaced proximal humeral fractures?
Abstract
Background: Proximal humeral fractures are mainly associated with osteoporosis and are becoming more common with the aging of our society. The best surgical approach for internal fixation of displaced proximal humeral fractures is still being debated.
Questions/purposes: In this prospective randomized study, we aimed to investigate whether the deltoid-split approach is superior to the deltopectoral approach with regard to (1) complication rate; (2) shoulder function (Constant score); and (3) pain (visual analog scale [VAS]) for internal fixation of displaced humeral fractures with a polyaxial locking plate.
Methods: We randomized 120 patients with proximal humeral fractures to receive one of these two approaches (60 patients for each approach). We prospectively documented demographic and perioperative data (sex, age, fracture type, hospital stay, operation time, and fluoroscopy time) as well as complications. Followup examinations were conducted at 6 weeks, 6 months, and 12 months postoperatively, including radiological and clinical evaluations (Constant score, activities of daily living, and pain [VAS]). Baseline and perioperative data were comparable for both approaches. The sample size was chosen to provide 80% power, but it reached only 68% as a result of the loss of followups to detect a 10-point difference on the Constant score, which we considered the minimum clinically important difference.
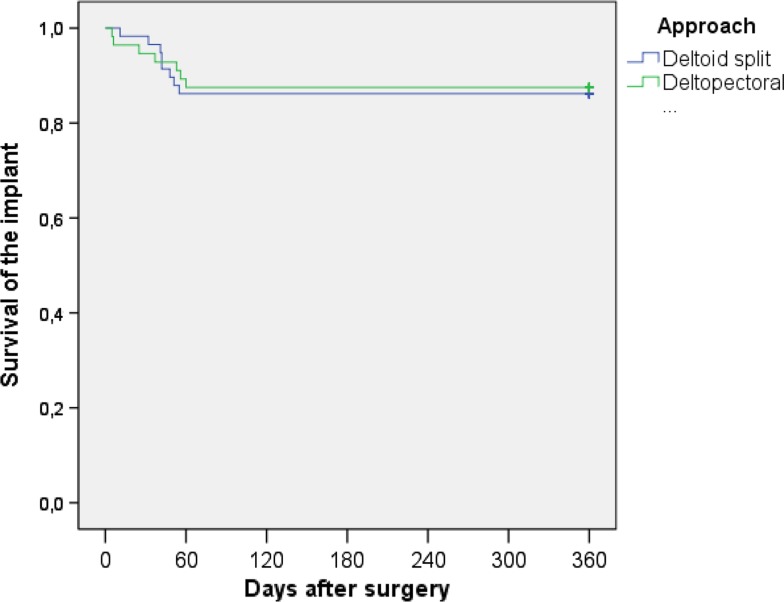
Results: Complications or reoperations between the approaches were not different. Eight patients in the deltoid-split group (14%) needed surgical revisions compared with seven patients in the deltopectoral group (13%; p = 1.00). Deltoid-split and deltopectoral approaches showed similar Constant scores 12 months postoperatively (Deltoid-split 81; 95% confidence interval [CI], 74-87 versus deltopectoral 73; 95% CI, 64-81; p = 0.13), and there were no differences between the groups in terms of pain at 1 year (deltoid-split 1.8; 95% CI, 1.2-1.4 versus deltopectoral 2.5; 95% CI, 1.7-3.2; p = 0.14). No learning-curve effects were noted; fluoroscopy use during surgery and function and pain scores during followups were similar among the first 30 patients and the next 30 patients treated in each group.
Conclusions: The treatment of proximal humeral fractures with a polyaxial locking plate is reliable using both approaches. For a definitive recommendation for one of these approaches, further studies with appropriate sample size are necessary.
Level of evidence: Level II, therapeutic study. See the Guidelines for Authors for a complete description of levels of evidence.
Figures




Comment in
-
CORR Insights®: Deltoid-split or deltopectoral approaches for the treatment of displaced proximal humeral fractures?Clin Orthop Relat Res. 2014 May;472(5):1586-8. doi: 10.1007/s11999-013-3449-x. Epub 2014 Jan 24. Clin Orthop Relat Res. 2014. PMID: 24464506 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
