

Hippocampal sparing radiotherapy for pediatric medulloblastoma: impact of treatment margins and treatment technique
- PMID: 24327585
- PMCID: PMC3956350
- DOI: 10.1093/neuonc/not225
Hippocampal sparing radiotherapy for pediatric medulloblastoma: impact of treatment margins and treatment technique
Abstract
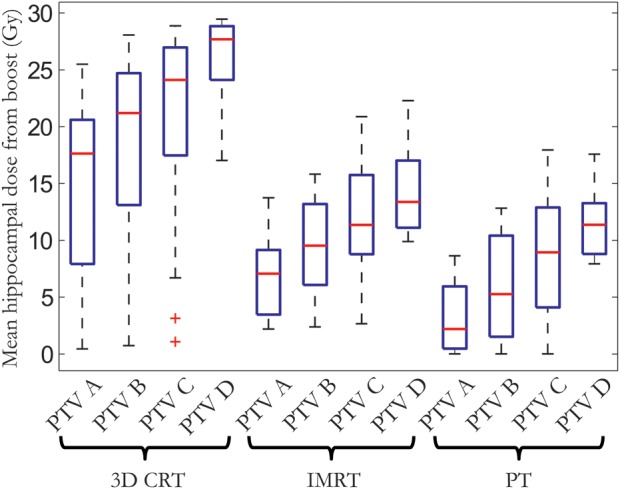
Background: We investigated how varying the treatment margin and applying hippocampal sparing and proton therapy impact the risk of neurocognitive impairment in pediatric medulloblastoma patients compared with current standard 3D conformal radiotherapy.
Methods: We included 17 pediatric medulloblastoma patients to represent the variability in tumor location relative to the hippocampal region. Treatment plans were generated using 3D conformal radiotherapy, hippocampal sparing intensity-modulated radiotherapy, and spot-scanned proton therapy, using 3 different treatment margins for the conformal tumor boost. Neurocognitive impairment risk was estimated based on dose-response models from pediatric CNS malignancy survivors and compared among different margins and treatment techniques.
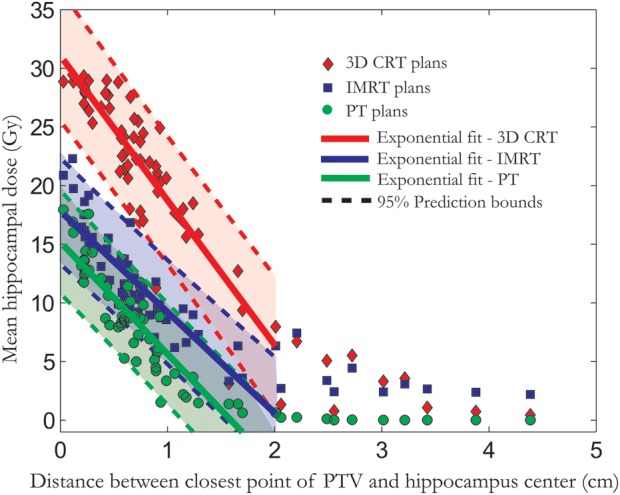
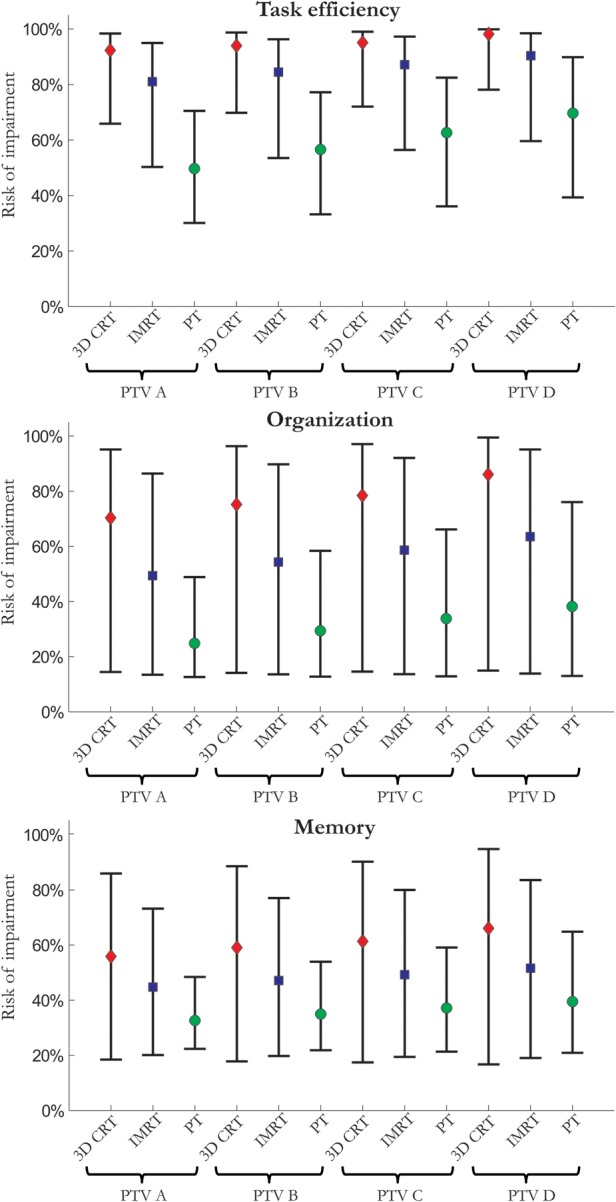
Results: Mean hippocampal dose and corresponding risk of cognitive impairment were decreased with decreasing treatment margins (P < .05). The largest risk reduction, however, was seen when applying hippocampal sparing proton therapy-the estimated risk of impaired task efficiency (95% confidence interval) was 92% (66%-98%), 81% (51%-95%), and 50% (30%-70%) for 3D conformal radiotherapy, intensity-modulated radiotherapy, and proton therapy, respectively, for the smallest boost margin and 98% (78%-100%), 90% (60%-98%), and 70% (39%-90%) if boosting the whole posterior fossa. Also, the distance between the closest point of the planning target volume and the center of the hippocampus can be used to predict mean hippocampal dose for a given treatment technique.
Conclusions: We estimate a considerable clinical benefit of hippocampal sparing radiotherapy. In choosing treatment margins, the tradeoff between margin size and risk of neurocognitive impairment quantified here should be considered.
Keywords: cognitive risk estimation; hippocampal sparing; medulloblastoma; tumor bed boost.
Figures
References
-
- Fossati P, Ricardi U, Orecchia R. Pediatric medulloblastoma: toxicity of current treatment and potential role of proton therapy. Cancer Treat Rev. 2009;35(1):79–96. - PubMed
-
- Lannering B, Rutkowski S, Doz F, et al. Hyperfractionated versus conventional radiotherapy followed by chemotherapy in standard-risk medulloblastoma: results from the randomized multicenter HIT-SIOP PNET 4 trial. J Clin Oncol. 2012;30(26):3187–3193. - PubMed
-
- Mulhern RK, Merchant TE, Gajjar A, Reddick WE, Kun LE. Late neurocognitive sequelae in survivors of brain tumours in childhood. Lancet Oncol. 2004;5(7):399–408. - PubMed
-
- Brown PD, Buckner JC, O'Fallon JR, et al. Effects of radiotherapy on cognitive function in patients with low-grade glioma measured by the Folstein mini-mental state examination. J Clin Oncol. 2003;21(13):2519–2524. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
