Review
doi: 10.5468/ogs.2013.56.3.143.
Epub 2013 May 16.
Breast diseases during pregnancy and lactation
Affiliations
- PMID: 24327995
- PMCID: PMC3784111
- DOI: 10.5468/ogs.2013.56.3.143
Item in Clipboard
Review
Breast diseases during pregnancy and lactation
Obstet Gynecol Sci.
2013 May.
Abstract
Breast is a typical female sexual physiologic organ that is influenced by steroid hormone from menarche until menopause. Therefore various diseases can be developed by continuous action of estrogen and progesterone. Breast diseases are mainly categorized as benign and malignant. It is very important to distinguish the malignancy from breast diseases. However, it is very difficult to diagnose malignancy in pregnant and lactating women even though the same breast diseases took place. Therefore, we will review breast diseases such as breast carcinoma during pregnancy and lactation.
Keywords: Breast disease; Lactation; Pregnancy.
Figures
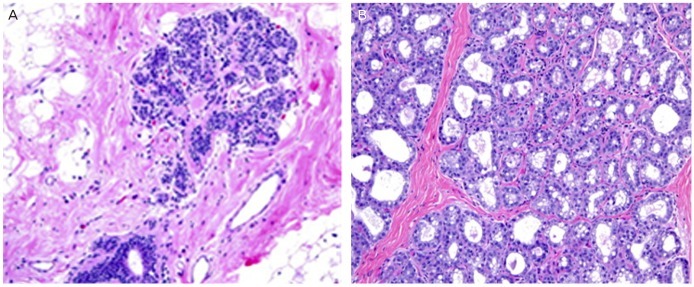
Changes of breast tissue during lactation. (A) Terminal duct-lobular unit in non-pregnancy (H&E, ×200). (B) Dilated lobular acini with vacuoles and secretions can be seen during lactation (H&E, ×200).
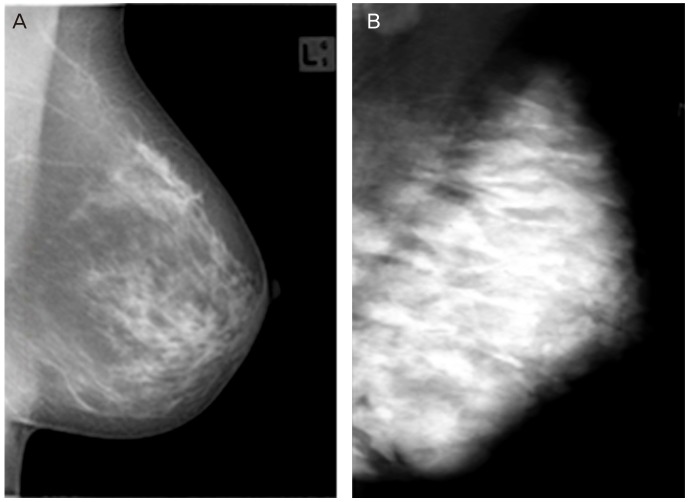
Mammographic changes during lactation. (A) Type 2 American College of Radiology classification shows before pregnancy. (B) Mammogram during lactation shows a marked diffuse increase in density.
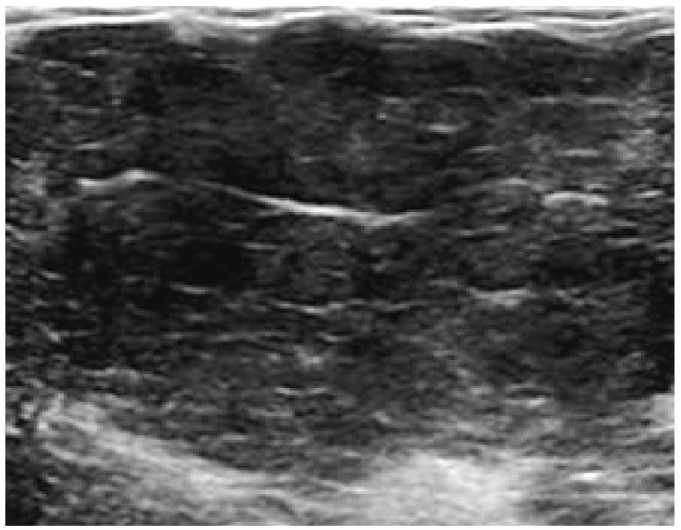
Typical ultrasonographic feature during pregnancy shows diffuse enlargement of the non-fatty glandular component and global hypoechogenicity.
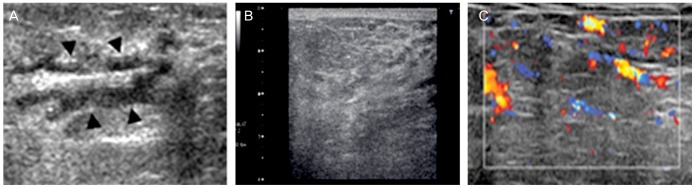
Ultrasonographic changes during lactation. (A) Ultrasound (US) image shows irregular margined, hypoechoic dilated duct (black arrowhead). (B) US image reveals diffuse enlargement of the glandular component with diffuse hyperechogenicity. (C) Color Doppler US image reveals increased vascularity.
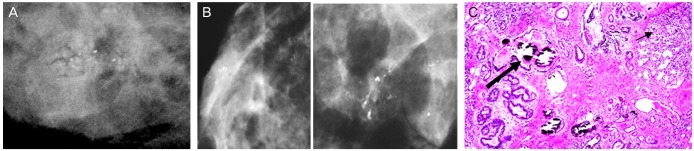
Microcalcifications during lactation. (A) Image shows new cluster of indeterminate asymmetric microcalcification. (B) Craniocaudal spot-compression magnification mammograms: several clusters of heterogeneous and granular calcifications. Some clusters display linear distribution. (C) Photomicrograph of histopathologic specimen: a Coarse microcalcification group is seen in the dilated duct. The relatively bigger microcalcification (thick arrow) shows in the single duct with homogeneous and eosiophillic feature. The smaller microcalcification (thin arrow) is seen in the lobule (H&E, ×50).
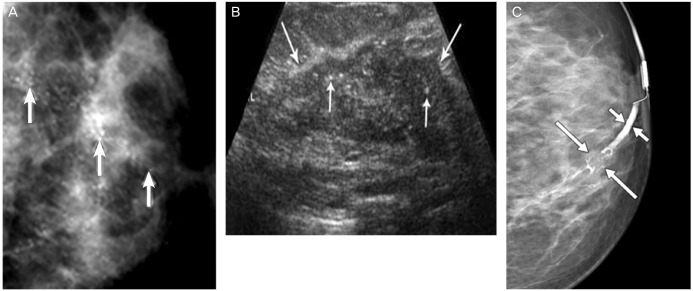
A woman who presented with palpable mass and bloody nipple discharge at 24 weeks of pregnancy. (A) Magnification view mammogram of left breast in craniocaudal projection: extensive pleomorphic microcalcifications (arrows). (B) Corresponding longitudinal ultrasound image: irregular solid hypoechoic mass (long arrows) with internal calcifications (short arrows) corresponding to mammographic finding. (C) A mammogram of 30 weeks of pregnant woman presented with bloody nipple discharge: Multilobulated filling defect (long arrows), which focally expands duct. Proximal duct is dilated (short arrows).
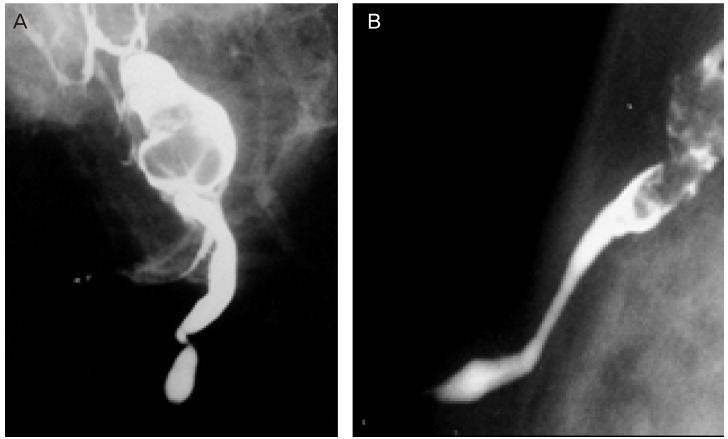
(A) The galactogram in a lactating woman who presented with bloody nipple discharge: lobular filling defect is seen which is expected to be intraductal papilloma. (B) The galactograms in patients with papillomatosis showing intra-ductal growth in a separate duct.
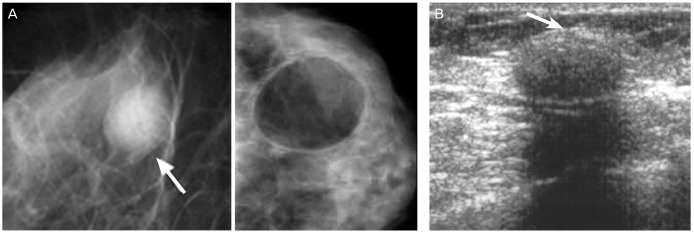
Pseudolipoma type galactocele. (A) Mammography shows a 1.5 cm oval circumscribed mass (arrow) at the subareolar region. (B) Sonography shows a 1.5 cm oval circumscribed hypoechoic nodule with posterior shadowing. An echogenic rim (arrow) can be seen at the anterior margin.
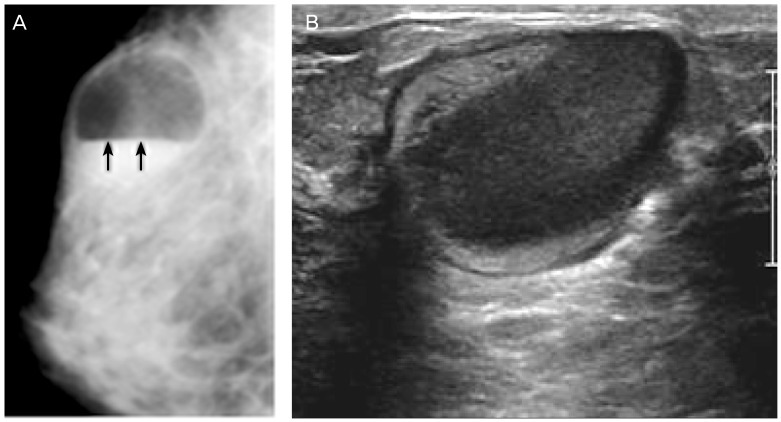
Galactocele with fat-fluid level. (A) An oval circumscribed cystic mass (arrows) with fat-fluid level is imaged in mammogram. (B) Ultrasound image shows the fat-fluid level with high echogenicity of lipid component and low echogenicity of fluid in the same patient.
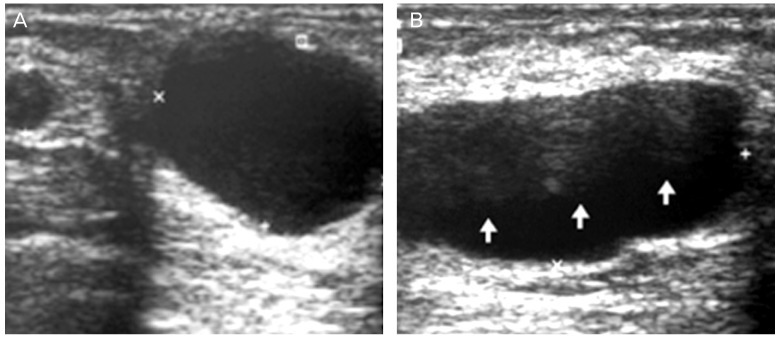
Galactocele 6 months post delivery which shows various features. (A) Ultrasound (US) image reveals 2 cystic mass: typical galactocele with homogenous anechoic, acoustic attenuation and lateral edge shadowing in bigger cyst. (B) US image shows the lobulated, fat-fluid (arrows) galactocele.
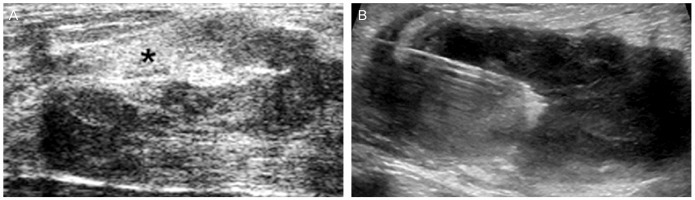
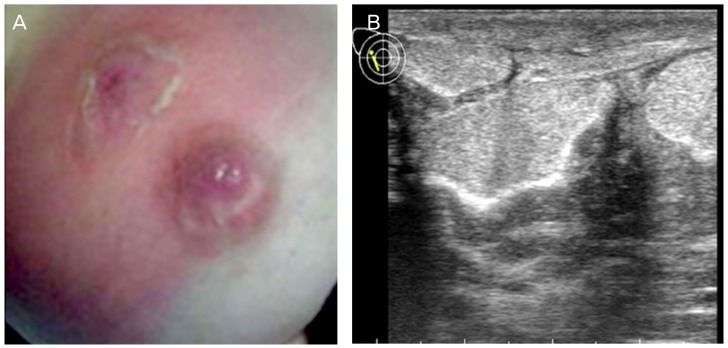
Infected galactocele: lactating woman who presented with reddish skin changes in the breast. (A) Ultrasound image shows a heterogeneous echoic, irregular margined collection which was suspicious of abscess. (B) Fine-needle aspiration and culture was performed.
Puerperal mastitis with abscess formation. (A) Lactational abscess grossly apparent secondary to flaming redness, hemorrhagic area, swelling, and peeling skin. (B) Ultrasound image shows large mass and purulent material was obtained by fine-needle aspiration.
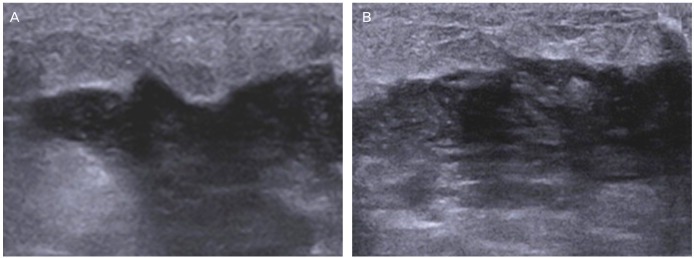
Ultrasound findings in puerperal mastitis. Early stage mastitis shows various features that is presented with thickness of skin and subcutaneous layer, and irregular border between subcutaneous layer and parenchyme. (A) US shows irregular margin and hypoechoic lesion. (B) If abscess is develop, hypoechoic or anechoic fluid collections can be seen. Irregular margin and echoic lesion can be also seen along with acoustic enhancement.
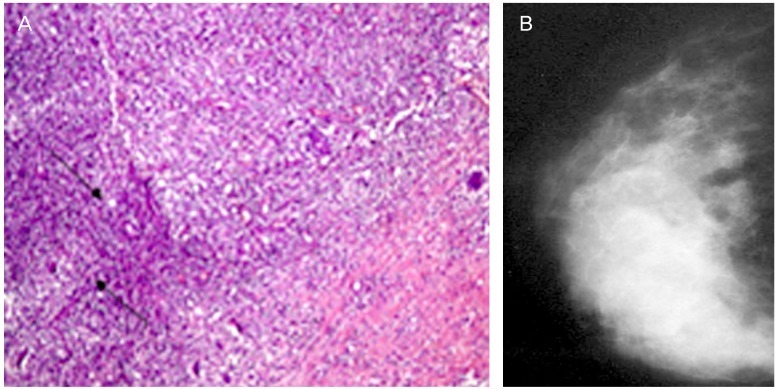
Granulomatous mastitis after pregnancy. (A) Photomicrograph (enlarged, H&E, ×10) shows epitheloid and giant cell granulomas (arrows) in polymorphous inflammatory infiltrate. (B) Mammogram shows irregular enhanced mass almost filled the right breast.
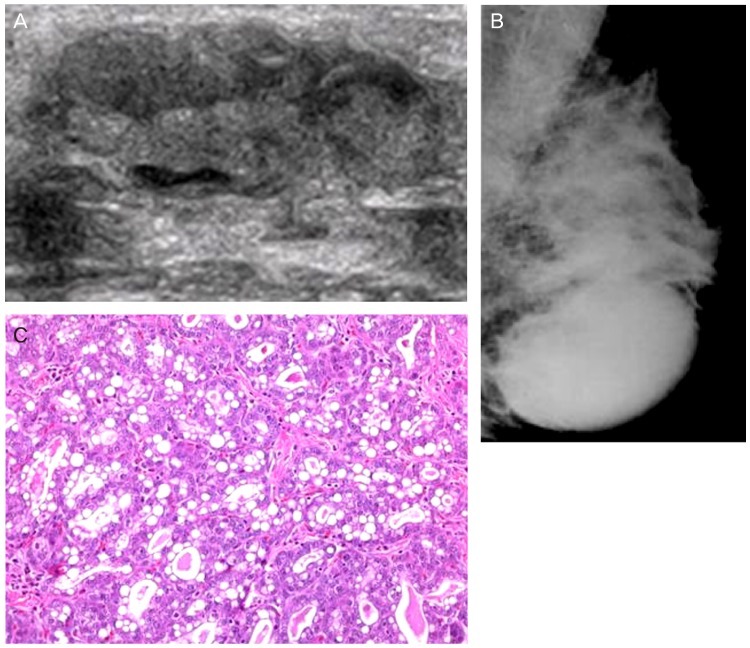
Lactating adenoma. (A) Ultrasound image demonstrates oval, well defined, regular margined mass. (B) Mammogram shows an oval circumscribed mass in the left lower breast. (C) The lobules are lined by actively secreting epithelial cells with vacuolated cytoplasm. Secretions may accumulate in the glands. The cells have basophilic cytoplasm, hyperchromatic nuclei with prominent nucleoli, and inconspicuous myoepithelial cell layer (H&E, ×400).
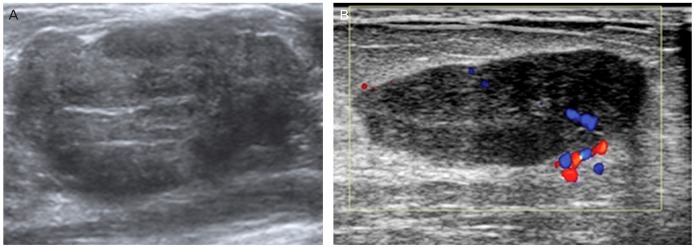
Fibroadenoma. (A) Aside from cystic lesion, fibroadenoma shows internal echogenicity and fibroadenoma can not be distinguished from malignant lesion perfectly. (B) Color Doppler Ultrasound image shows a fibroadenoma with increased vascularity and lobulated hypoechoic mass.
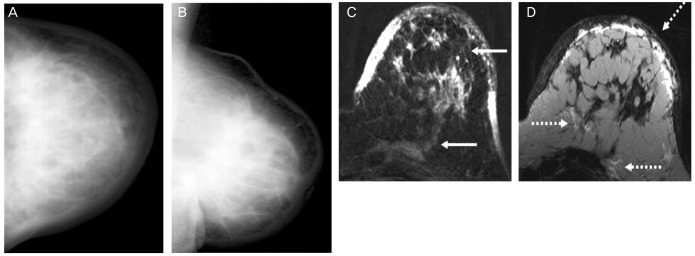
Inflammatory carcinoma during pregnancy. (A) Craniocaudal view. (B) Mediolateral-oblique view: mammogram shows a mark diffuse increase in parenchymal density with skin thickening. (C) Subtraction 1 minute after bolus injection-the diffuse enhancement infiltrating the skin and the pectoralis muscle (continuous arrows). (D) T2-weighted image-edema in a cutaneous/subcutaneous, diffuse and prepectoral localization (discontinuous arrows).
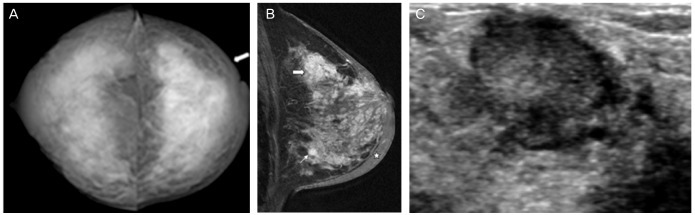
Pregnancy-associated breast cancer in a lactating woman who is presented with paeau d'orange skin. (A) Bilateral craniocaudal mammogram: severe dense breast with hypertrophic skin. (B) Mediolateral-oblique view: multiple mass (thick and thin arrows). (C) Ultrasound image in a lactating woman presented with palpable mass 9 months post delivery: it shows taller than wide mixed echogeic lesion revealed with invasive ductal carcinoma.
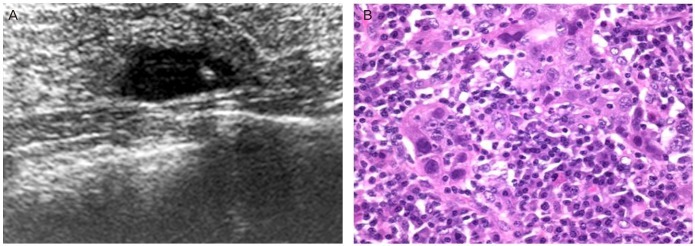
Atypical medullary carcinoma of the breast with cartilaginous metaplasia. (A) Ultrasound image reveals lobulated hypoechoic lesion in BRCA1 germline muation patient. (B) Higher magnification view of the previous slide shows the highly anaplastic tumor cells in a background of lymphoplasmacytic infiltrate (H&E, ×200).
References
-
- Kopans DB. Breast imaging. 2th ed. Philadelphia (PA): Lippincott-Raven; 1998.
-
- Salazar H, Tobon H, Josimovich JB. Developmental, gestational and postgestational modifications of the human breast. Clin Obstet Gynecol. 1975;18:113–137. - PubMed
-
- Rosen PP. Anatomic and physiologic morphology. In: Rosen PP, editor. Rosen's breast pathology. 2nd ed. Philadelphia (PA): Lippincott-Raven; 2001. pp. 1–21.
-
- Vorherr H. Human lactation and breast feeding. In: Larson BL, editor. Lactation: a comprehensive treatise. 2nd ed. New York (NY): Academic Press; 1978. pp. 182–280.
-
- Neville MC. Physiology of lactation. Clin Perinatol. 1999;26:251–279. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources