

The bronchiectasis severity index. An international derivation and validation study
- PMID: 24328736
- PMCID: PMC3977711
- DOI: 10.1164/rccm.201309-1575OC
The bronchiectasis severity index. An international derivation and validation study
Abstract
Rationale: There are no risk stratification tools for morbidity and mortality in bronchiectasis. Identifying patients at risk of exacerbations, hospital admissions, and mortality is vital for future research.
Objectives: This study describes the derivation and validation of the Bronchiectasis Severity Index (BSI).
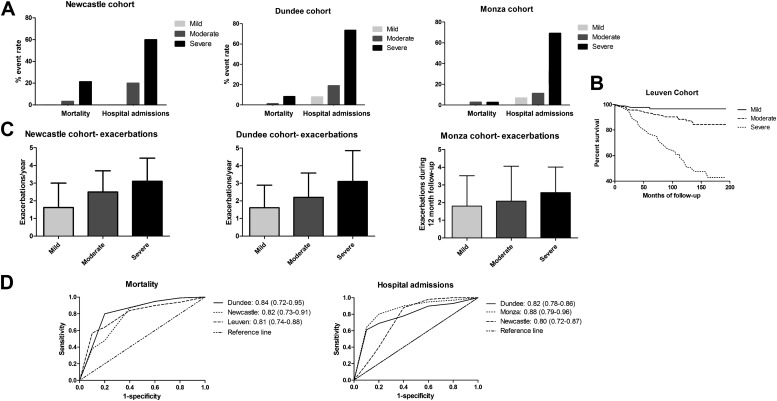
Methods: Derivation of the BSI used data from a prospective cohort study (Edinburgh, UK, 2008-2012) enrolling 608 patients. Cox proportional hazard regression was used to identify independent predictors of mortality and hospitalization over 4-year follow-up. The score was validated in independent cohorts from Dundee, UK (n = 218); Leuven, Belgium (n = 253); Monza, Italy (n = 105); and Newcastle, UK (n = 126).
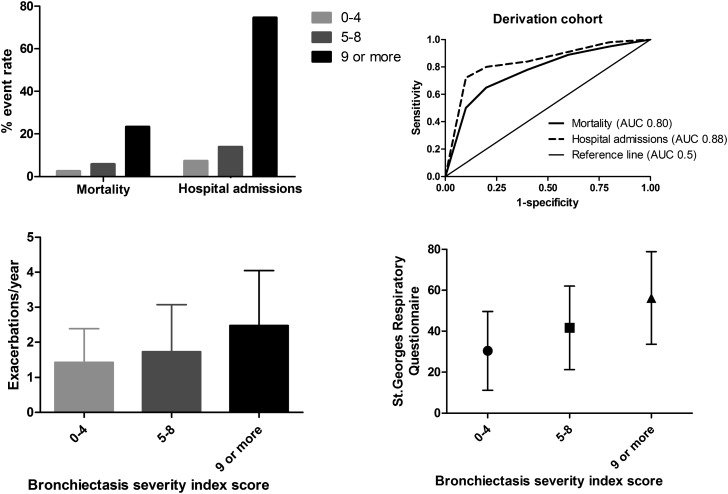
Measurements and main results: Independent predictors of future hospitalization were prior hospital admissions, Medical Research Council dyspnea score greater than or equal to 4, FEV1 < 30% predicted, Pseudomonas aeruginosa colonization, colonization with other pathogenic organisms, and three or more lobes involved on high-resolution computed tomography. Independent predictors of mortality were older age, low FEV1, lower body mass index, prior hospitalization, and three or more exacerbations in the year before the study. The derived BSI predicted mortality and hospitalization: area under the receiver operator characteristic curve (AUC) 0.80 (95% confidence interval, 0.74-0.86) for mortality and AUC 0.88 (95% confidence interval, 0.84-0.91) for hospitalization, respectively. There was a clear difference in exacerbation frequency and quality of life using the St. George's Respiratory Questionnaire between patients classified as low, intermediate, and high risk by the score (P < 0.0001 for all comparisons). In the validation cohorts, the AUC for mortality ranged from 0.81 to 0.84 and for hospitalization from 0.80 to 0.88.
Conclusions: The BSI is a useful clinical predictive tool that identifies patients at risk of future mortality, hospitalization, and exacerbations across healthcare systems.
Figures
Comment in
-
Bronchiectasis severity: time to score.Am J Respir Crit Care Med. 2014 Mar 1;189(5):508-9. doi: 10.1164/rccm.201401-0163ED. Am J Respir Crit Care Med. 2014. PMID: 24579834 No abstract available.
References
-
- Chalmers JD, Hill AT. Mechanisms of immune dysfunction and bacterial persistence in non-cystic fibrosis bronchiectasis. Mol Immunol. 2013;55:27–34. - PubMed
-
- Chalmers JD, Smith MP, McHugh BJ, Doherty C, Govan JR, Hill AT. Short- and long-term antibiotic treatment reduces airway and systemic inflammation in non-cystic fibrosis bronchiectasis. Am J Respir Crit Care Med. 2012;186:657–665. - PubMed
-
- Pasteur MC, Bilton D, Hill AT British Thoracic Society Bronchiectasis non-CF Guideline Group. British Thoracic Society guideline for non-CF bronchiectasis. Thorax. 2010;65:i1–i58. - PubMed
-
- McShane PJ, Naureckas ET, Tino G, Strek ME. Non-cystic fibrosis bronchiectasis. Am J Respir Crit Care Med. 2013;188:647–656. - PubMed
-
- Lange P, Marott JL, Vestbo J, Olsen KR, Ingebrigtsen TS, Dahl M, Nordestgaard BG. Prediction of the clinical course of chronic obstructive pulmonary disease, using the new GOLD classification: a study of the general population. Am J Respir Crit Care Med. 2012;186:975–981. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
