

The current use of Impella 2.5 in acute myocardial infarction complicated by cardiogenic shock: results from the USpella Registry
- PMID: 24329756
- PMCID: PMC4238821
- DOI: 10.1111/joic.12080
The current use of Impella 2.5 in acute myocardial infarction complicated by cardiogenic shock: results from the USpella Registry
Abstract
Objectives: To evaluate the periprocedural characteristics and outcomes of patients supported with Impella 2.5 prior to percutaneous coronary intervention (pre-PCI) versus those who received it after PCI (post-PCI) in the setting of cardiogenic shock (CS) complicating an acute myocardial infarction (AMI).
Background: Early mechanical circulatory support may improve outcome in the setting of CS complicating an AMI. However, the optimal timing to initiate hemodynamic support has not been well characterized.
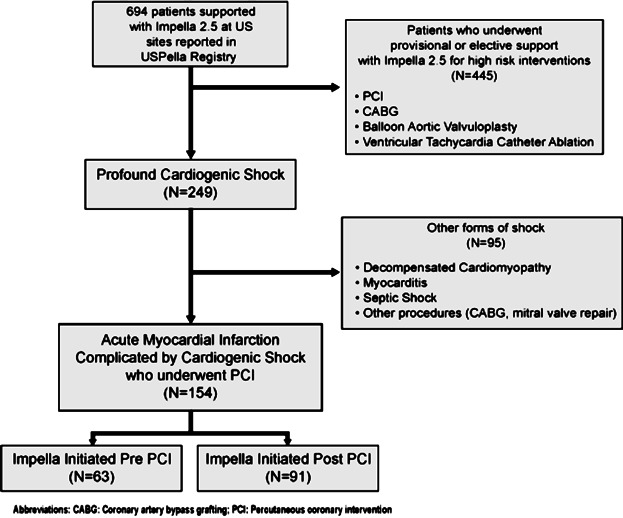
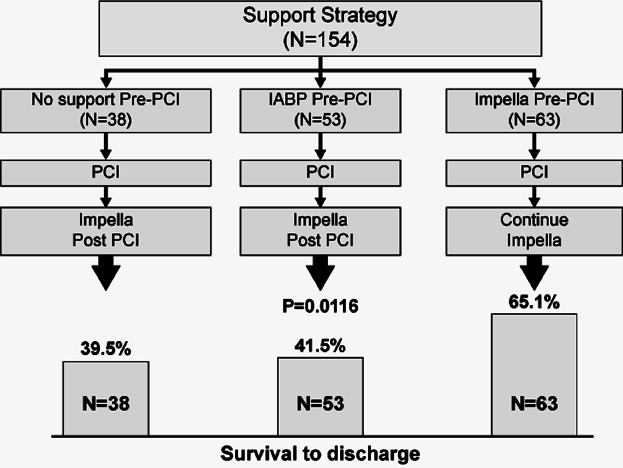
Methods: Data from 154 consecutive patients who underwent PCI and Impella 2.5 support from 38 US hospitals participating in the USpella Registry were included in our study. The primary end-point was survival to discharge. Secondary end-points included assessment of patients' hemodynamics and in-hospital complications. A multivariate regression model was used to identify independent predictors for mortality.
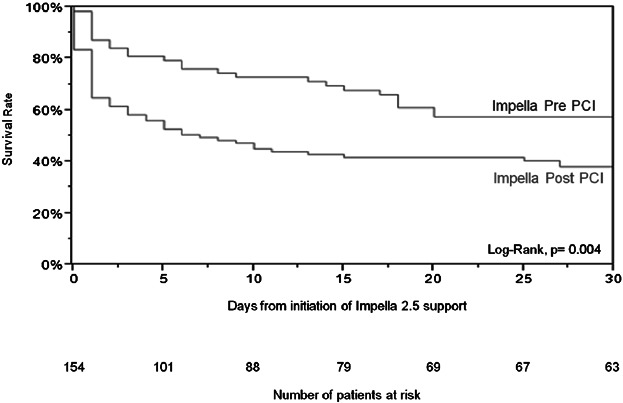
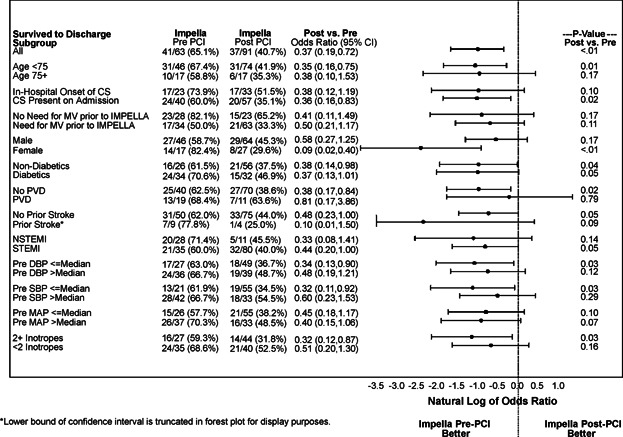
Results: Both groups were comparable except for diabetes (P = 0.02), peripheral vascular disease (P = 0.008), chronic obstructive pulmonary disease (P = 0.05), and prior stroke (P = 0.04), all of which were more prevalent in the pre-PCI group. Patients in the pre-PCI group had more lesions (P = 0.006) and vessels (P = 0.01) treated. These patients had also significantly better survival to discharge compared to patients in the post-PCI group (65.1% vs.40.7%, P = 0.003). Survival remained favorable for the pre-PCI group after adjusting for potential confounding variables. Initiation of support prior to PCI with Impella 2.5 was an independent predictor of in-hospital survival (Odds ratio 0.37, 95% confidence interval: 0.17-0.79, P = 0.01) in multivariate analysis. The incidence of in-hospital complications included in the secondary end-point was similar between the 2 groups.
Conclusions: The results of our study suggest that early initiation of hemodynamic support prior to PCI with Impella 2.5 is associated with more complete revascularization and improved survival in the setting of refractory CS complicating an AMI.
© 2013 The Authors. Journal of Interventional Cardiology published by Wiley Periodicals, Inc.
Figures
References
-
- Jeger RV, Radovanovic D, Hunziker PR, et al. Ten-year trends in the incidence and treatment of cardiogenic shock. Ann Intern Med. 2008;149:618–626. - PubMed
-
- Levine GN, Bates ER, Blankenship JC, et al. ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol. 2011;58:e44–e122. - PubMed
-
- Seyfarth M, Sibbing D, Bauer I, et al. A randomized clinical trial to evaluate the safety and efficacy of a percutaneous left ventricular assist device versus intra-aortic balloon pumping for treatment of cardiogenic shock caused by myocardial infarction. J Am Coll Cardiol. 2008;52:1584–1588. - PubMed
-
- O’Neill WW, Kleiman NS, Moses J, et al. A prospective, randomized clinical trial of hemodynamic support with Impella 2.5 versus intra-aortic balloon pump in patients undergoing high-risk percutaneous coronary intervention: The PROTECT II study. Circulation. 2012;126:1717–1727. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
