

Haemoglobinuria is associated with chronic kidney disease and its progression in patients with sickle cell anaemia
- PMID: 24329963
- PMCID: PMC3945021
- DOI: 10.1111/bjh.12690
Haemoglobinuria is associated with chronic kidney disease and its progression in patients with sickle cell anaemia
Abstract
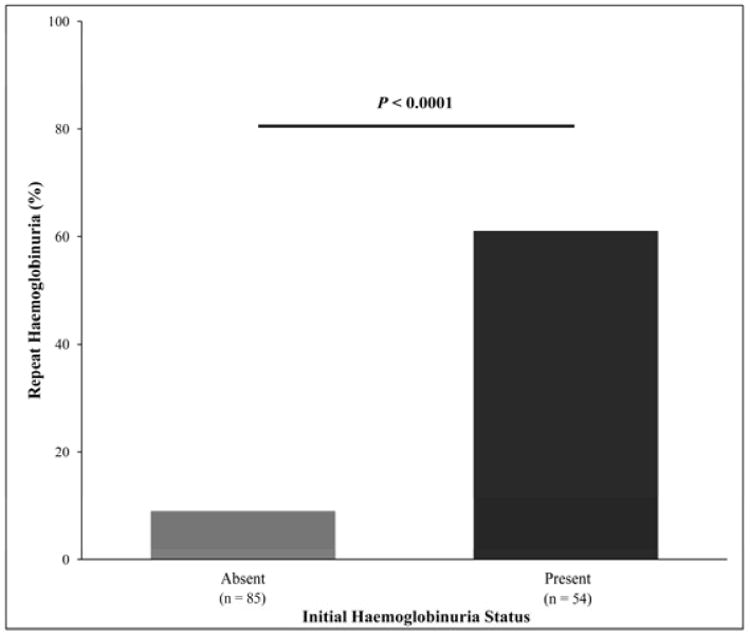
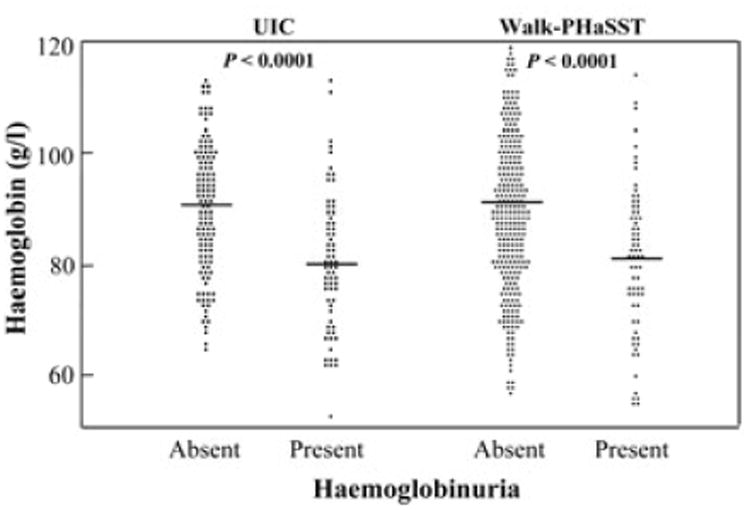
To evaluate the association between haemoglobinuria and chronic kidney disease (CKD) in sickle cell anaemia (SCA), we analysed 356 adult haemoglobin SS or Sβ(o) thalassaemia patients from the University of Illinois at Chicago (UIC) and 439 from the multi-centre Walk-Treatment of Pulmonary Hypertension and Sickle Cell Disease with Sildenafil Therapy (Walk-PHaSST) cohort. CKD was classified according to National Kidney Foundation Kidney Disease Outcomes Quality Initiatives guidelines. Haemoglobinuria, defined as positive haem on urine dipstick with absent red blood cells on microscopy, was confirmed by enzyme-linked immunosorbent assay in a subset of patients. The prevalence of CKD was 58% in the UIC cohort and 54% in the Walk-PHaSST cohort, and haemoglobinuria was observed in 36% and 20% of the patients, respectively. Pathway analysis in both cohorts indicated an independent association of lactate dehydrogenase with haemoglobinuria and, in turn, independent associations of haemoglobinuria and age with CKD (P < 0·0001). After a median of 32 months of follow-up in the UIC cohort, haemoglobinuria was associated with progression of CKD [halving of estimated glomerular filtration rate or requirement for dialysis; Hazard ratio (HR) 13·9, 95% confidence interval (CI) 1·7-113·2, P = 0·0012] and increasing albuminuria (HR 3·1, 95% CI: 1·3-7·7; logrank P = 0·0035). In conclusion haemoglobinuria is common in SCA and is associated with CKD, consistent with a role for intravascular haemolysis in the pathogenesis of renal dysfunction in SCA.
Keywords: albuminuria; haemoglobinuria; haemolysis; kidney disease; sickle cell.
© 2013 John Wiley & Sons Ltd.
Figures









References
-
- Abo-Zenah H, Moharram M, El Nahas AM. Cardiorenal risk prevalence in sickle cell hemoglobinopathy. Nephron Clin Pract. 2009;112:c98–c106. - PubMed
-
- Aleem A. Renal abnormalities in patients with sickle cell disease: a single center report from Saudi Arabia. Saudi J Kidney Dis Transpl. 2008;19:194–199. - PubMed
-
- Alvarez O, Lopez-Mitnik G, Zilleruelo G. Short-term follow-up of patients with sickle cell disease and albuminuria. Pediatr Blood Cancer. 2008;50:1236–1239. - PubMed
-
- Arlet JB, Ribeil JA, Chatellier G, Eladari D, De Seigneux S, Souberbielle JC, Friedlander G, de Montalembert M, Pouchot J, Prie D, Courbebaisse M. Determination of the best method to estimate glomerular filtration rate from serum creatinine in adult patients with sickle cell disease: a prospective observational cohort study. BMC Nephrol. 2012;13:83. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K23 HL098454/HL/NHLBI NIH HHS/United States
- P01 HL103455/HL/NHLBI NIH HHS/United States
- K24DK092290/DK/NIDDK NIH HHS/United States
- P01HL103455/HL/NHLBI NIH HHS/United States
- R01 HL098032/HL/NHLBI NIH HHS/United States
- R01HL111656/HL/NHLBI NIH HHS/United States
- KL2TR000048/TR/NCATS NIH HHS/United States
- R01HL098032/HL/NHLBI NIH HHS/United States
- L30 DK099990/DK/NIDDK NIH HHS/United States
- R01 HL096973/HL/NHLBI NIH HHS/United States
- R01HL096973/HL/NHLBI NIH HHS/United States
- K24 DK092290/DK/NIDDK NIH HHS/United States
- R01 HL111656/HL/NHLBI NIH HHS/United States
- K23HL098454/HL/NHLBI NIH HHS/United States
- KL2 TR000048/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
