

Procalcitonin-guided therapy in intensive care unit patients with severe sepsis and septic shock--a systematic review and meta-analysis
- PMID: 24330744
- PMCID: PMC4056085
- DOI: 10.1186/cc13157
Procalcitonin-guided therapy in intensive care unit patients with severe sepsis and septic shock--a systematic review and meta-analysis
Abstract
Introduction: Procalcitonin (PCT) algorithms for antibiotic treatment decisions have been studied in adult patients from primary care, emergency department, and intensive care unit (ICU) settings, suggesting that procalcitonin-guided therapy may reduce antibiotic exposure without increasing the mortality rate. However, information on the efficacy and safety of this approach in the most vulnerable population of critically ill patients with severe sepsis and septic shock is missing.
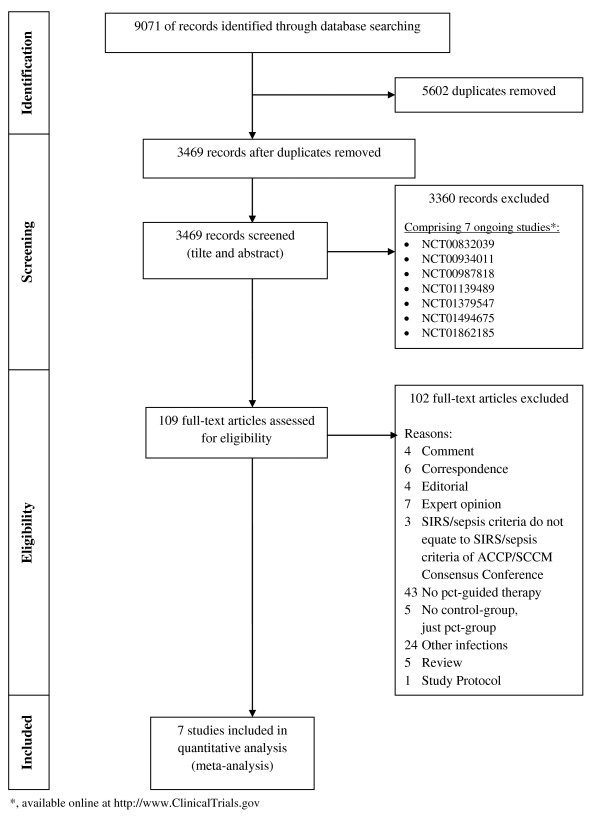
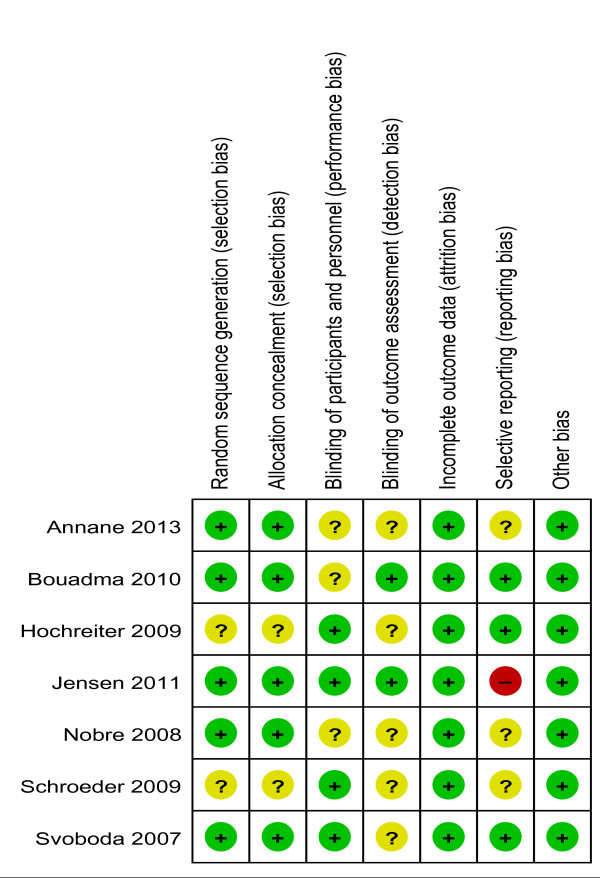
Method: Two reviewers independently performed a systematic search in PubMed, Embase, ISI Web of Knowledge, BioMed Central, ScienceDirect, Cochrane Central Register of Controlled Trials, http://www.ClinicalTrials.gov and http://www.ISRCTN.org. Eligible studies had to be randomized controlled clinical trials or cohort studies which compare procalcitonin-guided therapy with standard care in severe sepsis patients and report at least one of the following outcomes: hospital mortality, 28-day mortality, duration of antimicrobial therapy, length of stay in the intensive care unit or length of hospital stay. Disagreements about inclusion of studies and judgment of bias were solved by consensus.
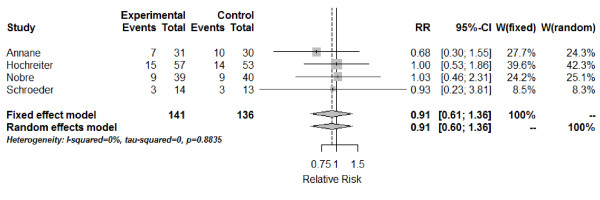
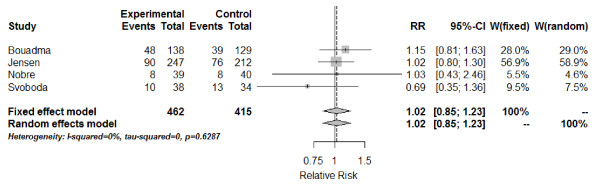
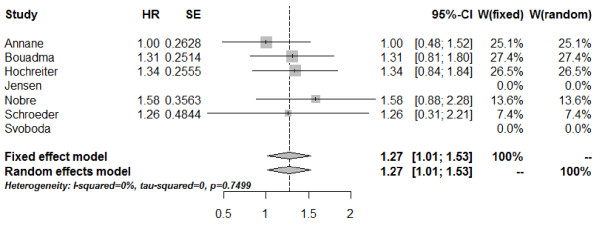
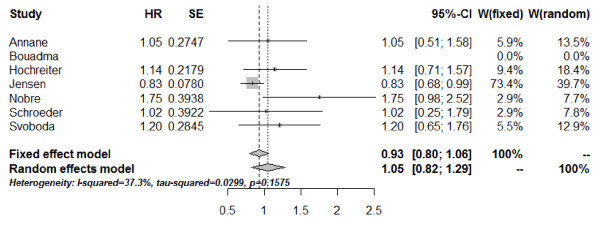
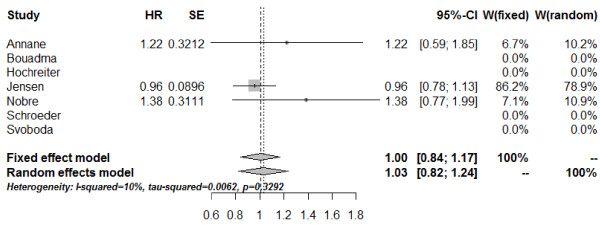
Results: Finally seven studies comprising a total of 1,075 patients with severe sepsis or septic shock were included in the meta-analysis. Both hospital mortality (RR [relative risk]: 0.91, 95%CI [confidence interval]: 0.61; 1.36) and 28-day mortality (RR: 1.02, 95%CI: 0.85; 1.23) were not different between procalcitonin-guided therapy and standard treatment groups. Duration of antimicrobial therapy was significantly reduced in favor of procalcitonin-guided therapy (HR [hazard ratio]: 1.27, 95%CI: 1.01; 1.53). Combined estimates of the length of stay in the ICU and in hospital did not differ between groups.
Conclusion: Procalcitonin-guided therapy is a helpful approach to guide antibiotic therapy and surgical interventions without a beneficial effect on mortality. The major benefit of PCT-guided therapy consists of a shorter duration of antibiotic treatment compared to standard care. Trials are needed to investigate the effect of PCT-guided therapy on mortality, length of ICU and in-hospital stay in severe sepsis patients.
Figures
Comment in
-
Using procalcitonin to guide antimicrobial duration in sepsis: asking the same questions will not bring different answers.Crit Care. 2014 May 13;18(3):142. doi: 10.1186/cc13870. Crit Care. 2014. PMID: 25032999 Free PMC article.
-
Procalcitonin-guided therapy in severe sepsis and septic shock.Crit Care. 2014 May 3;18(3):427. doi: 10.1186/cc13856. Crit Care. 2014. PMID: 25033407 Free PMC article. No abstract available.
-
Procalcitonin-guided therapy in severe sepsis and septic shock. Authors' response.Crit Care. 2014 May 3;18(3):427. Crit Care. 2014. PMID: 25473656 No abstract available.
References
-
- Engel C, Brunkhorst FM, Bone HG, Brunkhorst R, Gerlach H, Grond S, Gruendling M, Huhle G, Jaschinski U, John S, Mayer K, Oppert M, Olthoff D, Quintel M, Ragaller M, Rossaint R, Stuber F, Weiler N, Welte T, Bogatsch H, Hartog C, Loeffler M, Reinhart K. Epidemiology of sepsis in Germany: results from a national prospective multicenter study. Intensive Care Med. 2007;17:606–618. doi: 10.1007/s00134-006-0517-7. - DOI - PubMed
-
- Brunbuisson C, Doyon F, Carlet J, Dellamonica P, Gouin F, Lepoutre A, Mercier JC, Offenstadt G, Regnier B. Incidence, risk-factors, and outcome of severe sepsis and septic shock in adults - a multicenter prospective-study in intensive-care units. JAMA. 1995;17:968–974. doi: 10.1001/jama.1995.03530120060042. - DOI - PubMed
-
- Heublein S, Hartmann M, Hagel S, Hutagalung R, Brunkhorst FM. Epidemiology of sepsis in German hospitals derived from administrative databases. Infection. 2013;17:S71.
-
- Carrol ED, Thomson AP, Hart CA. Procalcitonin as a marker of sepsis. Int J Antimicrob Agents. 2002;17:1–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
