

Hemodynamic variables and progression of acute kidney injury in critically ill patients with severe sepsis: data from the prospective observational FINNAKI study
- PMID: 24330815
- PMCID: PMC4056430
- DOI: 10.1186/cc13161
Hemodynamic variables and progression of acute kidney injury in critically ill patients with severe sepsis: data from the prospective observational FINNAKI study
Abstract
Introduction: Knowledge of the association of hemodynamics with progression of septic acute kidney injury (AKI) is limited. However, some recent data suggest that mean arterial pressure (MAP) exceeding current guidelines (60-65 mmHg) may be needed to prevent AKI. We hypothesized that higher MAP during the first 24 hours in the intensive care unit (ICU), would be associated with a lower risk of progression of AKI in patients with severe sepsis.
Methods: We identified 423 patients with severe sepsis and electronically recorded continuous hemodynamic data in the prospective observational FINNAKI study. The primary endpoint was progression of AKI within the first 5 days of ICU admission defined as new onset or worsening of AKI by the Kidney Disease: Improving Global Outcomes (KDIGO) criteria. We evaluated the association of hemodynamic variables with this endpoint. We included 53724 10-minute medians of MAP in the analysis. We analysed the ability of time-adjusted MAP to predict progression of AKI by receiver operating characteristic (ROC) analysis.
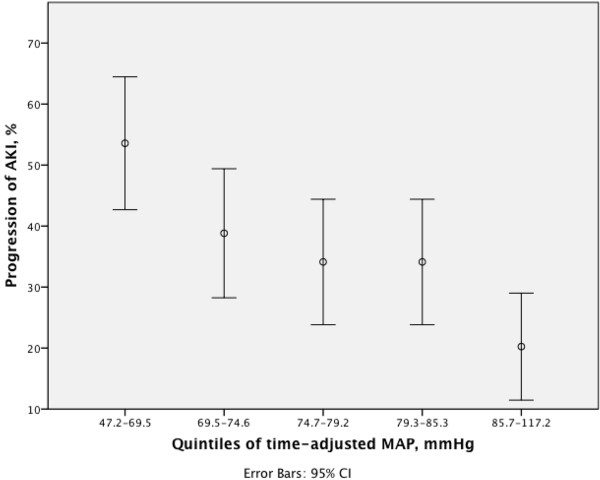
Results: Of 423 patients, 153 (36.2%) had progression of AKI. Patients with progression of AKI had significantly lower time-adjusted MAP, 74.4 mmHg [68.3-80.8], than those without progression, 78.6 mmHg [72.9-85.4], P < 0.001. A cut-off value of 73 mmHg for time-adjusted MAP best predicted the progression of AKI. Chronic kidney disease, higher lactate, higher dose of furosemide, use of dobutamine and time-adjusted MAP below 73 mmHg were independent predictors of progression of AKI.
Conclusions: The findings of this large prospective multicenter observational study suggest that hypotensive episodes (MAP under 73 mmHg) are associated with progression of AKI in critically ill patients with severe sepsis.
Figures


References
-
- Oppert M, Engel C, Brunkhorst FM, Bogatsch H, Reinhart K, Frei U, Eckardt KU, Loeffler M, John S. German Competence Network Sepsis (Sepnet) Acute renal failure in patients with severe sepsis and septic shock–a significant independent risk factor for mortality: results from the German prevalence study. Nephrol Dial Transplant. 2008;17:904–909. - PubMed
-
- Bagshaw SM, Lapinsky S, Dial S, Arabi Y, Dodek P, Wood G, Ellis P, Guzman J, Marshall J, Parrillo JE, Skrobik Y, Kumar A. Cooperative Antimicrobial Therapy of Septic Shock (CATSS) Database Research Group. Acute kidney injury in septic shock: clinical outcomes and impact of duration of hypotension prior to initiation of antimicrobial therapy. Intensive Care Med. 2009;17:871–881. doi: 10.1007/s00134-008-1367-2. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
