

Impairment of subendocardial perfusion reserve and oxidative metabolism in nonischemic dilated cardiomyopathy
- PMID: 24331202
- PMCID: PMC3945036
- DOI: 10.1016/j.cardfail.2013.10.010
Impairment of subendocardial perfusion reserve and oxidative metabolism in nonischemic dilated cardiomyopathy
Abstract
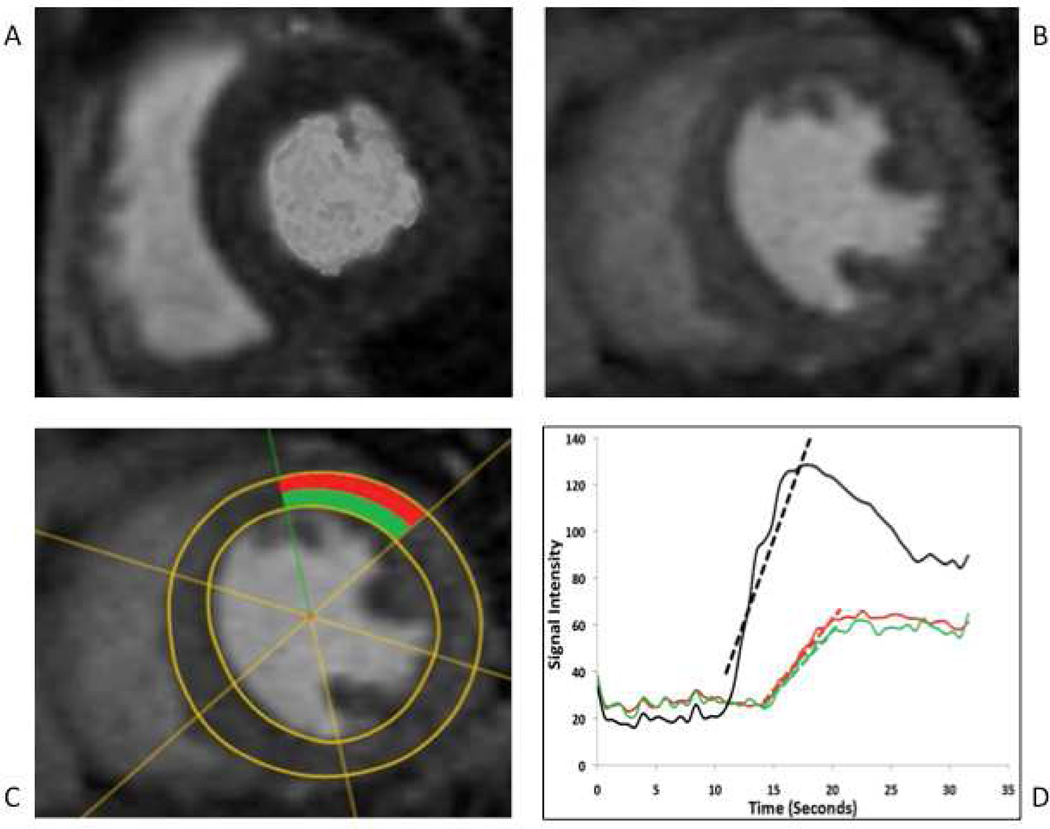
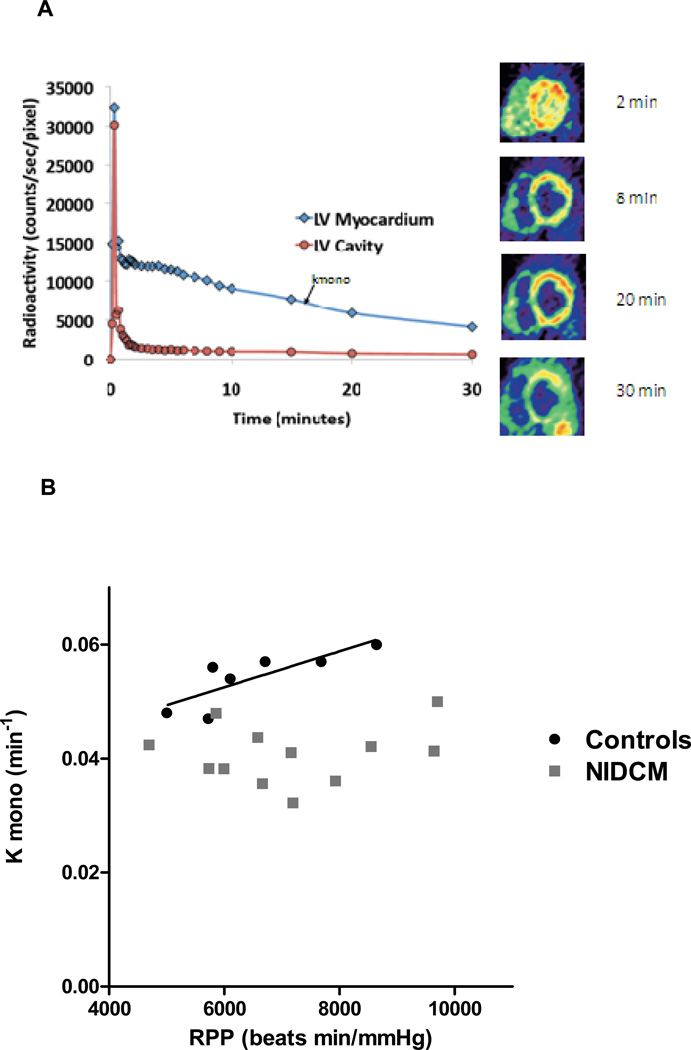
Background: Cardiac magnetic resonance (CMR) and [(11)C]acetate positron emission tomography (PET) were used to assess the hypothesis that patients with nonischemic dilated cardiomyopathy (NIDCM) have decreased subendocardial perfusion reserve and impaired oxidative metabolism, consistent with the concept of "energy starvation" in heart failure (HF).
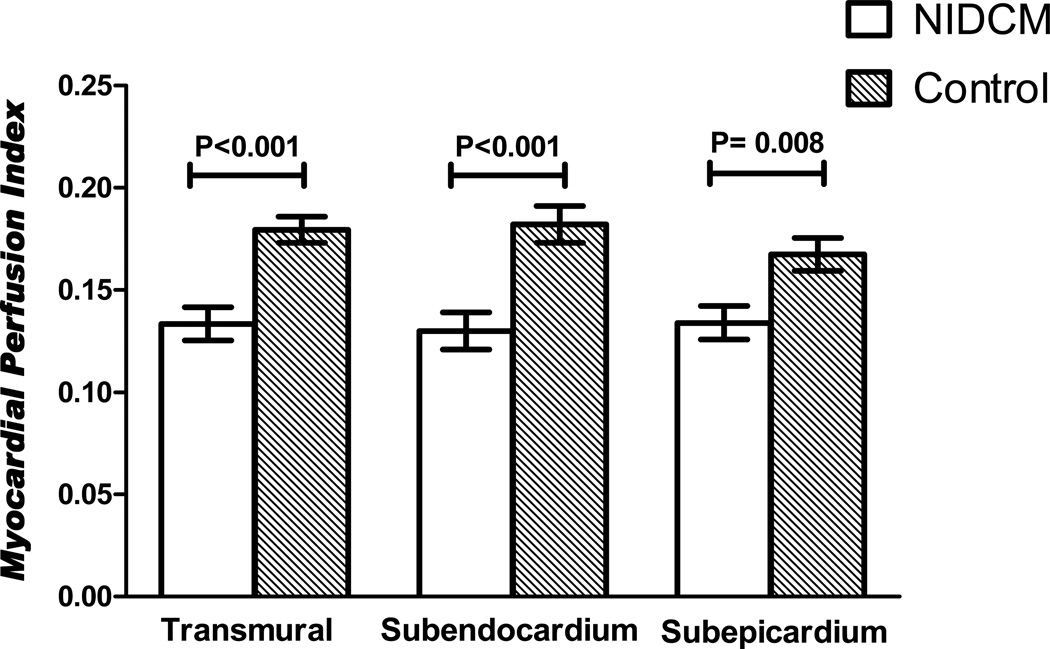
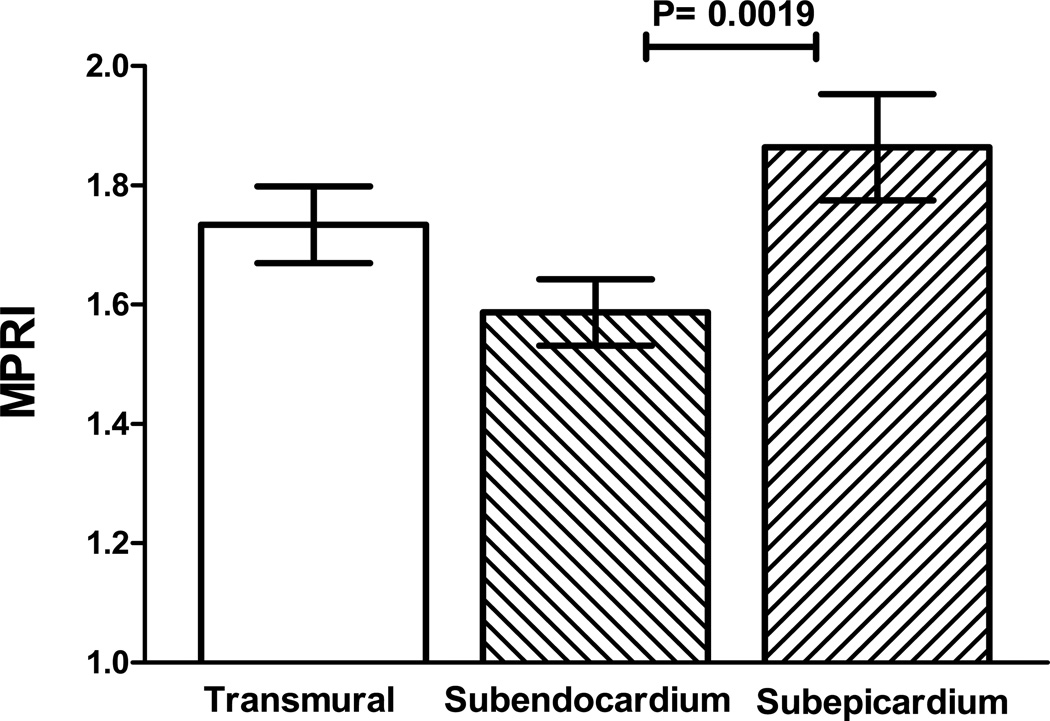
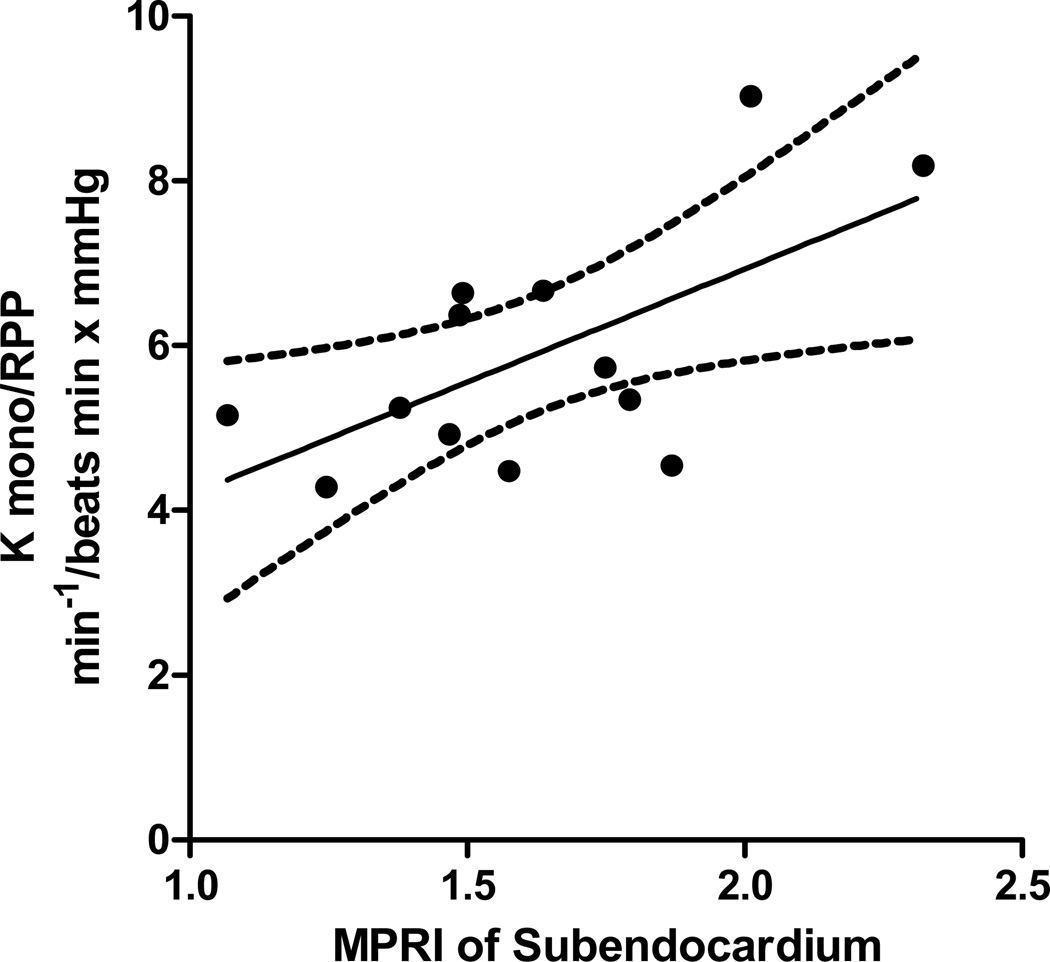
Methods and results: CMR myocardial perfusion was evaluated in 13 NIDCM patients and 15 control subjects with coronary risk factors and normal myocardial perfusion. The NIDCM patients underwent [(11)C]acetate PET. The myocardial perfusion index (MPI) was calculated as the normalized rate of myocardial signal augmentation following gadolinium contrast injection. Hyperemic transmural, subendocardial, and subepicardial MPI were reduced in NIDCM compared with control subjects [0.13 vs 0.18 (P < .001), 0.13 vs 0.17 (P < .001), and 0.13 vs 0.17 (P = .008), respectively]. The subendocardial perfusion reserve was 1.59 ± 0.21 vs 1.86 ± 0.32 for the subepicardium (P = .002), demonstrating reduced perfusion reserve. The myocardial oxidative metabolic rate (kmono) per unit demand (rate-pressure product) was reduced in proportion to perfusion reserve (P = .02) CONCLUSIONS: Impaired subendocardial perfusion reserve in NIDCM confirmed results previously attained only in animal models. Impaired perfusion and impaired oxidative metabolism are consistent with subendocardial energy starvation in HF.
Trial registration: ClinicalTrials.gov NCT00574119.
Keywords: CMR; fibrosis; heart failure; myocardial blood flow; oxidative metabolism.
Published by Elsevier Inc.
Figures
References
-
- [accessed May 25th 2013]; http://depts.washington.edu/shfm/app.php,
-
- Katz AM. The myocardium in congestive heart failure. Am J Cardiol. 1989;63:12A–16A. - PubMed
-
- Tsagalou EP, Anastasiou-Nana M, Agapitos E, Gika A, Drakos SG, Terrovitis JV, et al. Depressed coronary flow reserve is associated with decreased myocardial capillary density in patients with heart failure due to idiopathic dilated cardiomyopathy. J Am Coll Cardiol. 2008;52:1391–1398. - PubMed
-
- Katz AM. Cardiomyopathy of overload. A major determinant of prognosis in congestive heart failure. N Engl J Med. 1990;322:100–110. - PubMed
-
- Olson RE, Schwartz WB. Myocardial metabolism in congestive heart failure. Medicine (Baltimore) 1951;30:21–41. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
