

Valid measures of periodic leg movements (PLMs) during a suggested immobilization test using the PAM-RL leg activity monitors require adjusting detection parameters for noise and signal in each recording
- PMID: 24332046
- PMCID: PMC3921115
- DOI: 10.1016/j.sleep.2013.08.788
Valid measures of periodic leg movements (PLMs) during a suggested immobilization test using the PAM-RL leg activity monitors require adjusting detection parameters for noise and signal in each recording
Abstract
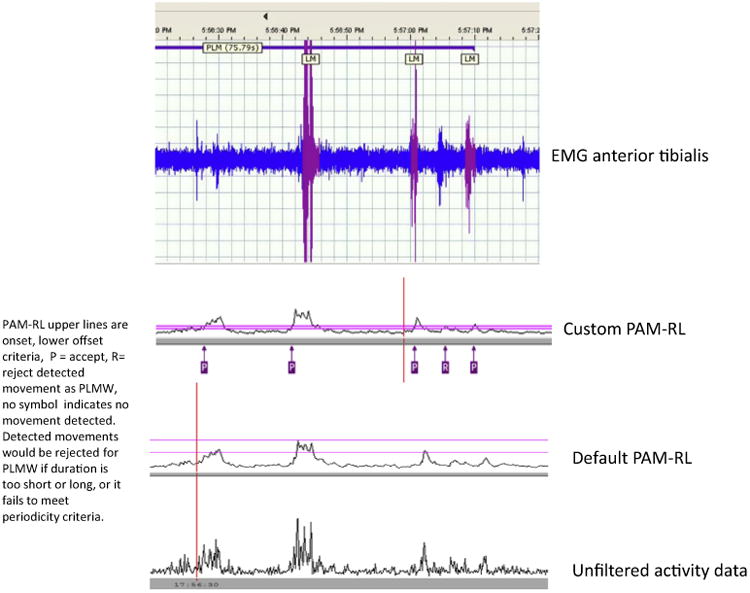
Objective and background: Individuals with restless legs syndrome (RLS) (Willis-Ekbom disease [WED]) usually have periodic leg movements (PLMs). The suggested immobilization test (SIT) measures sensory and motor features of WED during wakefulness. Surface electromyogram (EMG) recordings of the anterior tibialis (AT) are used as the standard for counting PLMs. However, due to several limitations, leg activity meters such as the PAM-RL were advanced as a potential substitute. In our study, we assessed the validity of the measurements of PLM during wakefulness (PLMW) in the SIT for PAM-RL using both default and custom detection threshold parameters compared to AT EMG.
Methods: Data were obtained from 39 participants who were diagnosed with primary WED and who were on stable medication as part of another study using the SIT to repeatedly evaluate WED symptoms over 6-12 months. EMG recordings and PAM-RL, when available, were used to detect PLMW for each SIT. Complete PAM-RL and polysomnography (PSG) EMG data were available for 253 SITs from that study. The default PAM-RL (dPAM-RL) detected leg movements based on manufacturer's noise (resting) and signal (movement) amplitude criteria developed to accurately detect PLM during sleep (PLMS). The custom PAM-RL (cPAM-RL) similarly detected leg movements except the noise and movement detection parameters were adjusted to match the PAM-RL data for each SIT.
Results: The distributions of the differences between either dPAM-RL or cPAM-RL and EMG PLMW were strongly leptokurtic (Kurtosis >2) with many small differences and a few unusually large differences. These distributions are better described by median and quartile ranges than mean and standard deviation. Despite an adequate correlation (r=0.66) between the dPAM-RL and EMG recordings, the dPAM-RL on average significantly underscored the number of PLMW (median: quartiles=-13: -51.2, 0.0) and on Bland-Altman plots had a significant magnitude bias with greater underscoring for larger average PLMW/h. There also was an adequate correlation (r=0.70) between cPAM-RL and EMG but with minimal underscoring of PLMW (median quartiles=0.0; -20, 10) and no significant magnitude bias. Two scorers independently scoring 13% of the SITs showed an adequate interscorer reliability of 0.96-0.98.
Conclusions: Our study confirms our expectation that measuring PLMW in a SIT using dPAM-RL is not valid and that adjustments to the detection threshold criteria are required. The PAM-RL, using parameters customized for each SIT provided a valid and reliable measure of PLMW with minimal magnitude bias compared to the AT EMG recordings.
Keywords: Leg activity monitors; PAM-RL; Periodic leg movements during wakefulness (PLMW); Polysomnography; Restless Legs Syndrome (RLS); Suggested immobilization test (SIT); Willis Ekbom disease (WED).
Copyright © 2013 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures




References
-
- Allen RP, Picchietti D, Hening WA, Trenkwalder C, Walters AS, Montplaisir J. Restless legs syndrome: diagnostic criteria, special considerations, and epidemiology. A report from the restless legs syndrome diagnosis and epidemiology workshop at the National Institutes of Health. Sleep Med. 2003;4:101–19. - PubMed
-
- Montplaisir J, Boucher S, Poirier G, Lavigne G, Lapierre O, Lesperance P. Clinical, polysomnographic, and genetic characteristics of restless legs syndrome: a study of 133 patients diagnosed with new standard criteria. Mov Disord. 1997;12:61–5. - PubMed
-
- Montplaisir J, Boucher S, Nicolas A, Lesperance P, Gosselin A, Rompre P, et al. Immobilization tests and periodic leg movements in sleep for the diagnosis of restless leg syndrome. Mov Disord. 1998;13:324–9. - PubMed
-
- Michaud M, Paquet J, Lavigne G, Desautels A, Montplaisir J. Sleep laboratory diagnosis of restless legs syndrome. Eur Neurol. 2002;48:108–13. - PubMed
-
- Zucconi M, Manconi M, Ferini Strambi L. Aetiopathogenesis of restless legs syndrome. Neurol Sci. 2007;28(Suppl. 1):S47–52. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
