

Minimally invasive fibrillating mitral valve replacement for patients with advanced cardiomyopathy: a safe and effective approach to treat a complex problem
- PMID: 24332110
- PMCID: PMC4050032
- DOI: 10.1016/j.jtcvs.2013.10.062
Minimally invasive fibrillating mitral valve replacement for patients with advanced cardiomyopathy: a safe and effective approach to treat a complex problem
Abstract
Objective: The optimal management of mitral regurgitation (MR) in patients with cardiomyopathy has been controversial. Minimally invasive fibrillating mitral valve replacement (mini-MVR) might limit postoperative morbidity and mortality by minimizing recurrent MR. We hypothesized that mini-MVR with complete chordal sparing would offer low mortality and halt left ventricular (LV) remodeling in patients with severe cardiomyopathy and severe MR.
Methods: From January 2006 to August 2009, 65 patients with an LV ejection fraction (LVEF) of ≤35% underwent mini-MVR. The demographic, echocardiographic, and clinical outcomes were analyzed.
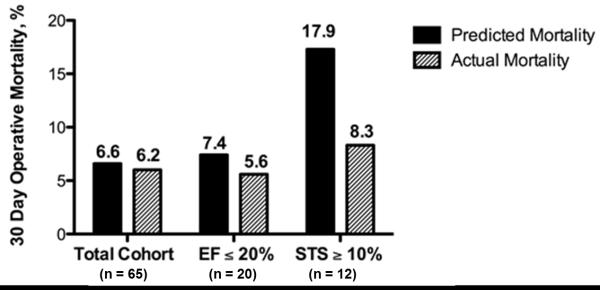
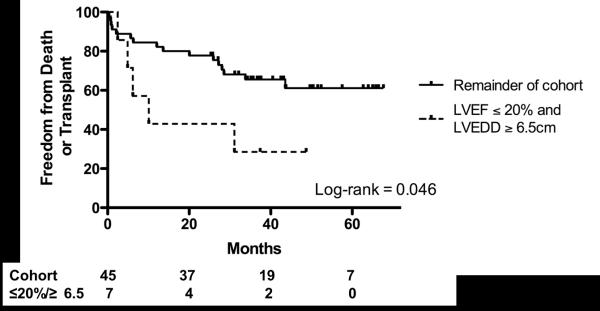
Results: The operative mortality compared with the Society of Thoracic Surgeons-predicted mortality was 6.2% versus 6.6%. It was 5.6% versus 7.4% for patients with an LVEF of ≤20% and 8.3% versus 17.9% among patients with a Society of Thoracic Surgeons-predicted mortality of ≥10%. At a median follow-up of 17 months, no recurrent MR or change in the LV dimensions or LVEF had developed, but the right ventricular systolic pressure had decreased (P=.02). At the first postoperative visit and latest follow-up visit, the New York Heart Association class had decreased from 3.0±0.6 to 1.7±0.7 and 2.0±1.0, respectively (P<.0001 for both). Patients with an LVEF of ≤20% and LV end-diastolic diameter of ≥6.5 cm were more likely to meet a composite of death, transplantation, or LV assist device insertion (P=.046).
Conclusions: Our results have shown that mini-MVR is safe in patients with advanced cardiomyopathy and resulted in no recurrent MR, stabilization of the LVEF and LV dimensions, and a decrease in right ventricular systolic pressure. This mini-MVR technique can be used to address severe MR in patients with advanced cardiomyopathy.
Copyright © 2014 The American Association for Thoracic Surgery. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Mehra MR, Reyes P, Benitez RM, Zimrin D, Gammie JS. Surgery for severe mitral regurgitation and left ventricular failure: what do we really know? J Card Fail. 2008 Mar;14(2):145–50. - PubMed
-
- Acker MA, Bolling S, Shemin R, et al. Mitral valve surgery in heart failure: insights from the Acorn Clinical Trial. J Thorac Cardiovasc Surg. 2006 Sep;132(3):568–77. 77 e1–4. - PubMed
-
- Di Salvo TG, Acker MA, Dec GW, Byrne JG. Mitral valve surgery in advanced heart failure. J Am Coll Cardiol. 2010 Jan 26;55(4):271–82. - PubMed
-
- Hung J, Papakostas L, Tahta SA, et al. Mechanism of recurrent ischemic mitral regurgitation after annuloplasty: continued LV remodeling as a moving target. Circulation. 2004 Sep 14;110(11 Suppl 1):II85–90. - PubMed
-
- McGee EC, Jr., Gillinov AM, Blackstone EH, et al. Recurrent mitral regurgitation after annuloplasty for functional ischemic mitral regurgitation. J Thorac Cardiovasc Surg. 2004;128(6):916. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
