

Sputum neutrophil counts are associated with more severe asthma phenotypes using cluster analysis
- PMID: 24332216
- PMCID: PMC4040309
- DOI: 10.1016/j.jaci.2013.10.011
Sputum neutrophil counts are associated with more severe asthma phenotypes using cluster analysis
Abstract
Background: Clinical cluster analysis from the Severe Asthma Research Program (SARP) identified 5 asthma subphenotypes that represent the severity spectrum of early-onset allergic asthma, late-onset severe asthma, and severe asthma with chronic obstructive pulmonary disease characteristics. Analysis of induced sputum from a subset of SARP subjects showed 4 sputum inflammatory cellular patterns. Subjects with concurrent increases in eosinophil (≥2%) and neutrophil (≥40%) percentages had characteristics of very severe asthma.
Objective: To better understand interactions between inflammation and clinical subphenotypes, we integrated inflammatory cellular measures and clinical variables in a new cluster analysis.
Methods: Participants in SARP who underwent sputum induction at 3 clinical sites were included in this analysis (n = 423). Fifteen variables, including clinical characteristics and blood and sputum inflammatory cell assessments, were selected using factor analysis for unsupervised cluster analysis.
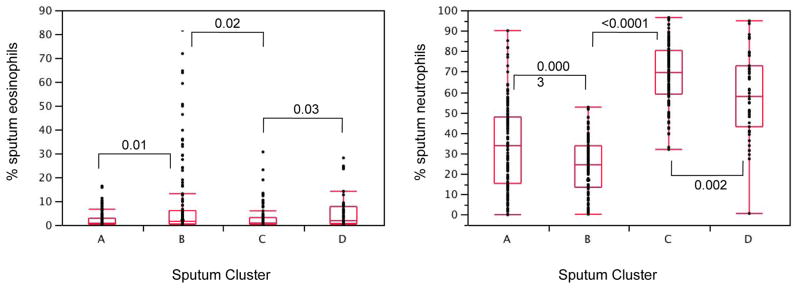
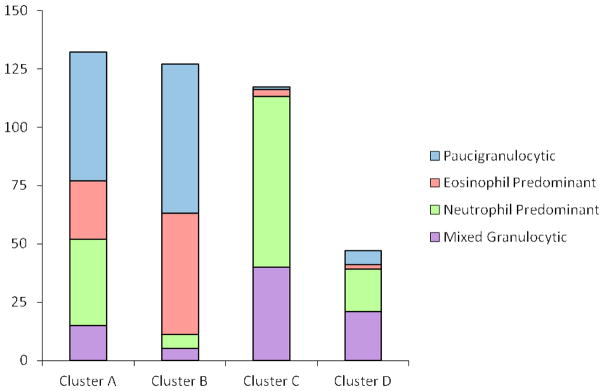
Results: Four phenotypic clusters were identified. Cluster A (n = 132) and B (n = 127) subjects had mild-to-moderate early-onset allergic asthma with paucigranulocytic or eosinophilic sputum inflammatory cell patterns. In contrast, these inflammatory patterns were present in only 7% of cluster C (n = 117) and D (n = 47) subjects who had moderate-to-severe asthma with frequent health care use despite treatment with high doses of inhaled or oral corticosteroids and, in cluster D, reduced lung function. The majority of these subjects (>83%) had sputum neutrophilia either alone or with concurrent sputum eosinophilia. Baseline lung function and sputum neutrophil percentages were the most important variables determining cluster assignment.
Conclusion: This multivariate approach identified 4 asthma subphenotypes representing the severity spectrum from mild-to-moderate allergic asthma with minimal or eosinophil-predominant sputum inflammation to moderate-to-severe asthma with neutrophil-predominant or mixed granulocytic inflammation.
Keywords: Severe Asthma Research Program; cluster analysis; eosinophils; neutrophils; phenotype; severe asthma; sputum.
Published by Mosby, Inc.
Figures
References
-
- National Asthma Education and Prevention Program. Expert Panel Report 3. Guidelines for the diagnosis and management of asthma. Bethesda, MD: National Institutes of Health; Heart, Lung and Blood Institute; 2007. [accessed on April 15, 2013]. No. 07-4051. Available at http://www.nhlbi.nih.gov/guidelines/asthma.
-
- Bateman ED, Hurd SS, Barnes PJ, Bousquet J, Drazen JM, FitzGerald M, et al. Global strategy for asthma management and prevention: GINA executive summary. Eur Respir J. 2008;31:143–78. - PubMed
-
- Proceedings of the ATS workshop on refractory asthma: current understanding, recommendations, and unanswered questions. American Thoracic Society. Am J Respir Crit Care Med. 2000;162:2341–51. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
