

Cardiac resynchronization therapy and AV optimization increase myocardial oxygen consumption, but increase cardiac function more than proportionally
- PMID: 24332598
- PMCID: PMC3919205
- DOI: 10.1016/j.ijcard.2013.10.026
Cardiac resynchronization therapy and AV optimization increase myocardial oxygen consumption, but increase cardiac function more than proportionally
Abstract
Background: The mechanoenergetic effects of atrioventricular delay optimization during biventricular pacing ("cardiac resynchronization therapy", CRT) are unknown.
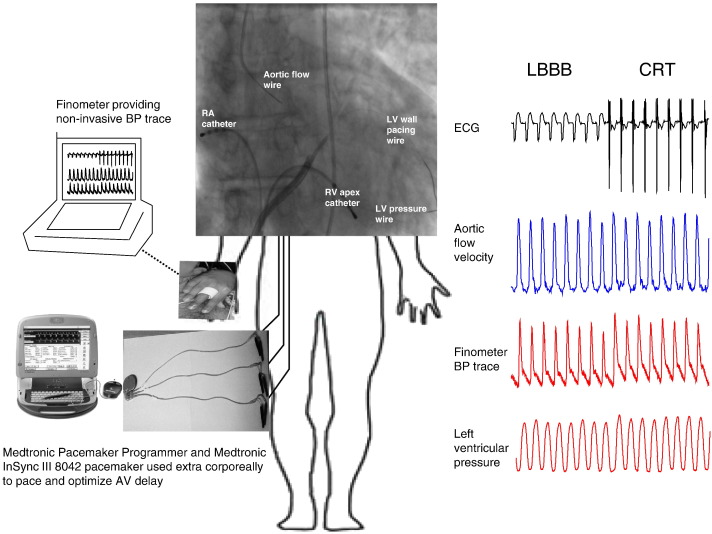
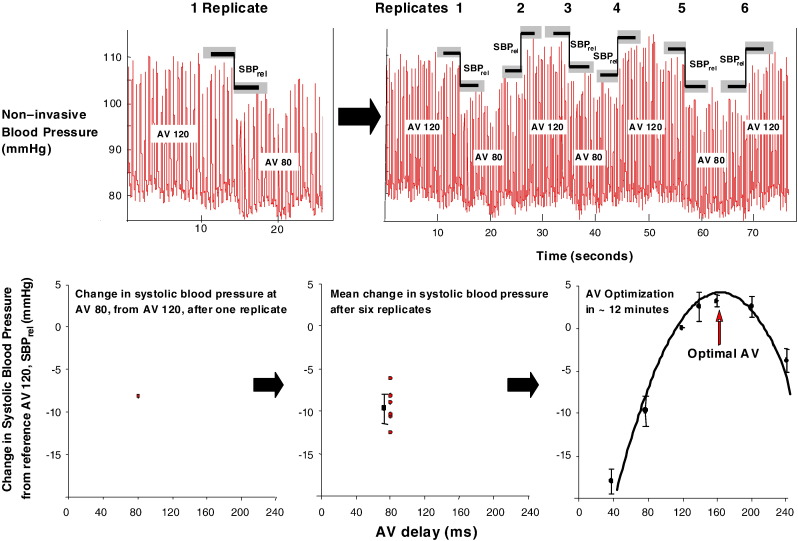
Methods: Eleven patients with heart failure and left bundle branch block (LBBB) underwent invasive measurements of left ventricular (LV) developed pressure, aortic flow velocity-time-integral (VTI) and myocardial oxygen consumption (MVO2) at 4 pacing states: biventricular pacing (with VV 0 ms) at AVD 40 ms (AV-40), AVD 120 ms (AV-120, a common nominal AV delay), at their pre-identified individualised haemodynamic optimum (AV-Opt); and intrinsic conduction (LBBB).
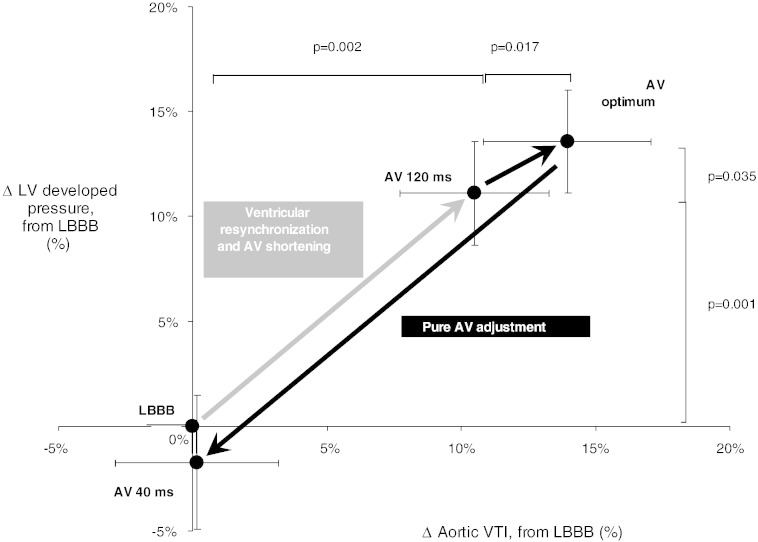
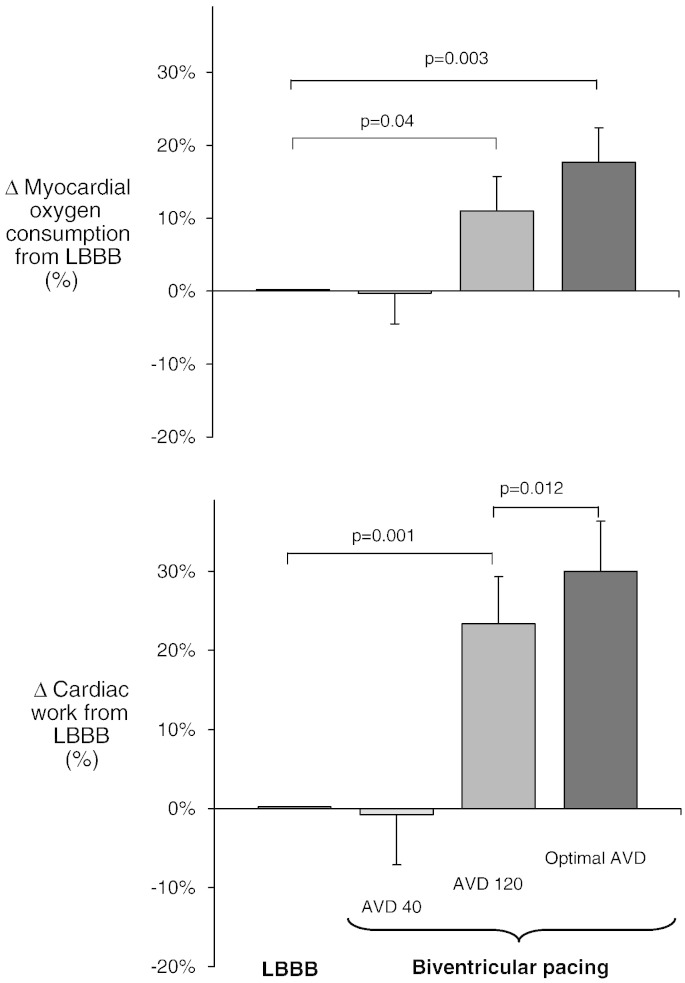
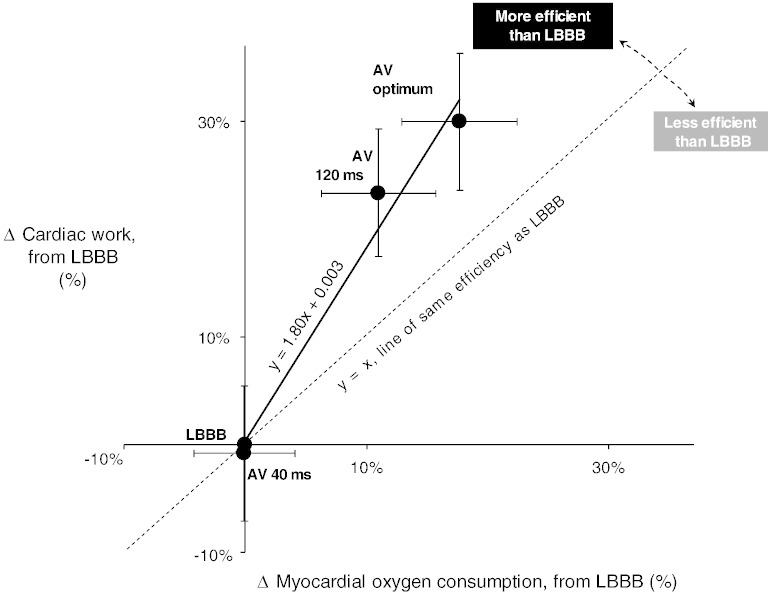
Results: AV-120, relative to LBBB, increased LV developed pressure by a mean of 11(SEM 2)%, p=0.001, and aortic VTI by 11(SEM 3)%, p=0.002, but also increased MVO2 by 11(SEM 5)%, p=0.04. AV-Opt further increased LV developed pressure by a mean of 2(SEM 1)%, p=0.035 and aortic VTI by 4(SEM 1)%, p=0.017. MVO2 trended further up by 7(SEM 5)%, p=0.22. Mechanoenergetics at AV-40 were no different from LBBB. The 4 states lay on a straight line for Δexternal work (ΔLV developed pressure × Δaortic VTI) against ΔMVO2, with slope 1.80, significantly >1 (p=0.02).
Conclusions: Biventricular pacing and atrioventricular delay optimization increased external cardiac work done but also myocardial oxygen consumption. Nevertheless, the increase in cardiac work was ~80% greater than the increase in oxygen consumption, signifying an improvement in cardiac mechanoenergetics. Finally, the incremental effect of optimization on external work was approximately one-third beyond that of nominal AV pacing, along the same favourable efficiency trajectory, suggesting that AV delay dominates the biventricular pacing effect - which may therefore not be mainly "resynchronization".
Keywords: Biventricular pacing; Myocardial oxygen consumption; Optimization.
© 2013. Published by Elsevier Ireland Ltd. All rights reserved.
Figures
Similar articles
-
Improvement in coronary blood flow velocity with acute biventricular pacing is predominantly due to an increase in a diastolic backward-travelling decompression (suction) wave.Circulation. 2012 Sep 11;126(11):1334-44. doi: 10.1161/CIRCULATIONAHA.111.075606. Epub 2012 Aug 1. Circulation. 2012. PMID: 22855569 Clinical Trial.
-
Calculation of effective VV interval facilitates optimization of AV delay and VV interval in cardiac resynchronization therapy.Heart Rhythm. 2007 Jan;4(1):75-82. doi: 10.1016/j.hrthm.2006.09.007. Epub 2006 Sep 9. Heart Rhythm. 2007. PMID: 17198994
-
Acute biventricular hemodynamic effects of cardiac resynchronization therapy in right bundle branch block.Heart Rhythm. 2018 Oct;15(10):1525-1532. doi: 10.1016/j.hrthm.2018.05.017. Epub 2018 May 23. Heart Rhythm. 2018. PMID: 29800750
-
Assessment of mechanical dyssynchrony in cardiac resynchronization therapy.Dan Med J. 2014 Dec;61(12):B4981. Dan Med J. 2014. PMID: 25441737 Review.
-
The Emerging Role of Cardiac Conduction System Pacing as a Treatment for Heart Failure.Curr Heart Fail Rep. 2020 Oct;17(5):288-298. doi: 10.1007/s11897-020-00474-y. Curr Heart Fail Rep. 2020. PMID: 32857325 Free PMC article. Review.
Cited by
-
Successful Cardiac Resynchronization Therapy Reduces Negative Septal Work in Patient-Specific Models of Dyssynchronous Heart Failure.bioRxiv [Preprint]. 2024 May 14:2024.05.13.593804. doi: 10.1101/2024.05.13.593804. bioRxiv. 2024. Update in: PLoS Comput Biol. 2024 Oct 10;20(10):e1012150. doi: 10.1371/journal.pcbi.1012150. PMID: 38798676 Free PMC article. Updated. Preprint.
-
The impact of cardiac resynchronization therapy on routine laboratory parameters.Interv Med Appl Sci. 2017 Mar;9(1):1-8. doi: 10.1556/1646.9.2017.1.01. Interv Med Appl Sci. 2017. PMID: 28932489 Free PMC article.
-
Successful cardiac resynchronization therapy reduces negative septal work in patient-specific models of dyssynchronous heart failure.PLoS Comput Biol. 2024 Oct 10;20(10):e1012150. doi: 10.1371/journal.pcbi.1012150. eCollection 2024 Oct. PLoS Comput Biol. 2024. PMID: 39388481 Free PMC article.
-
Effects of Epicardial and Endocardial Cardiac Resynchronization Therapy on Coronary Flow: Insights From Wave Intensity Analysis.J Am Heart Assoc. 2015 Dec 17;4(12):e002626. doi: 10.1161/JAHA.115.002626. J Am Heart Assoc. 2015. PMID: 26679935 Free PMC article.
-
Changes in contractility determine coronary haemodynamics in dyssynchronous left ventricular heart failure, not vice versa.Int J Cardiol Heart Vasc. 2018 Apr 4;19:8-13. doi: 10.1016/j.ijcha.2018.03.002. eCollection 2018 Jun. Int J Cardiol Heart Vasc. 2018. PMID: 29946557 Free PMC article.
References
-
- Leclercq C., Cazeau S., Le Breton H. Acute hemodynamic effects of biventricular DDD pacing in patients with end-stage heart failure. J Am Coll Cardiol. 1998;32:1825–1831. - PubMed
-
- Auricchio A., Ding J., Spinelli J.C. Cardiac resynchronization therapy restores optimal atrioventricularmechanical timing in heart failure patients with ventricular conduction delay. J Am Coll Cardiol. 2002;39:1163–1169. - PubMed
-
- Kass D.A., Chen C.H., Curry C. Improved left ventricular mechanics from acute VDD pacing in patients with dilated cardiomyopathy and ventricular conduction delay. Circulation. 1999;30:1567–1573. - PubMed
-
- Butter C., Auricchio A., Stellbrink C. Pacing Therapy for Chronic Heart Failure II Study Group. Effect of resynchronization therapy stimulation site on the systolic function of heart failure patients. Circulation. 2001;18:3026–3029. - PubMed
-
- van Gelder B.M., Bracke F.A., Meijer A., Pijls N.H. The hemodynamic effect of intrinsic conduction during left ventricular pacing as compared to biventricular pacing. J Am Coll Cardiol. 2005;20:2305–2310. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
