

Erythrocytapheresis compared with whole blood phlebotomy for the treatment of hereditary haemochromatosis
- PMID: 24333062
- PMCID: PMC3934269
- DOI: 10.2450/2013.0128-13
Erythrocytapheresis compared with whole blood phlebotomy for the treatment of hereditary haemochromatosis
Abstract
Background: Hereditary haemochromatosis may result in severe organ damage which can be prevented by therapy. We studied the possible advantages and disadvantages of erythrocytapheresis as compared with phlebotomy in patients with hereditary haemochromatosis.
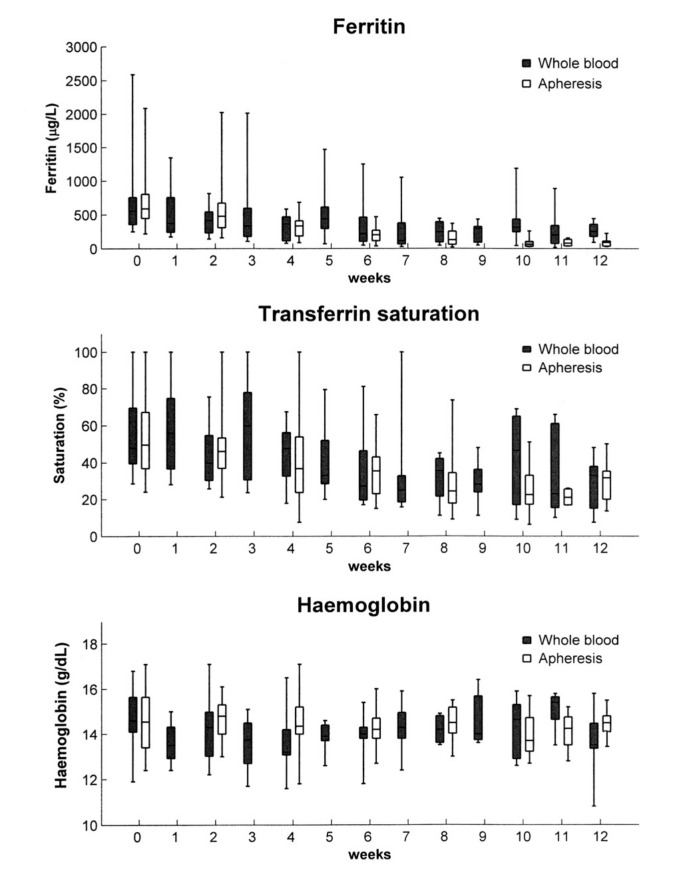
Materials and methods: In a prospective, randomised, open-label study, patients with hereditary haemochromatosis were randomised to bi-weekly apheresis or weekly whole blood phlebotomy. Primary end-points were decrease in ferritin levels and transferrin saturation. Secondary endpoints were decrease in haemoglobin levels, discomfort during the therapeutic procedure, costs and technicians' working time.
Results: Sixty-two patients were included. Thirty patients were randomised to apheresis and 32 to whole blood phlebotomy. Initially, ferritin levels declined more rapidly in the apheresis group, and the difference became statistically highly significant at 11 weeks; however, time to normalisation of ferritin level was equal in the two groups. We observed no significant differences in decline of transferrin saturation, haemoglobin levels or discomfort. The mean cumulative technician time consumption until the ferritin level reached 50 μg/L was longer in the apheresis group, but the difference was not statistically significant. The cumulative costs for materials until achievement of the desired ferritin levels were three-fold higher in the apheresis group.
Conclusion: Treatment of hereditary haemochromatosis with erythrocytapheresis instead of whole blood phlebotomy results in a more rapid initial decline in ferritin levels and a reduced number of procedures per patient, but not in earlier achievement of target ferritin level. The frequency of discomfort was equally low with the two methods. The costs and, probably, technician time consumption were higher in the apheresis group.
Figures
Similar articles
-
Rusfertide for the treatment of iron overload in HFE-related haemochromatosis: an open-label, multicentre, proof-of-concept phase 2 trial.Lancet Gastroenterol Hepatol. 2023 Dec;8(12):1118-1128. doi: 10.1016/S2468-1253(23)00250-9. Epub 2023 Oct 17. Lancet Gastroenterol Hepatol. 2023. PMID: 37863080 Clinical Trial.
-
Course of iron parameters in HFE-hemochromatosis patients during initial treatment with erythrocytapheresis compared to phlebotomy.J Clin Apher. 2016 Dec;31(6):564-570. doi: 10.1002/jca.21451. Epub 2016 Feb 16. J Clin Apher. 2016. PMID: 26878994
-
[Erythrocytapheresis for hereditary haemochromatosis].Ned Tijdschr Geneeskd. 2012;156(26):A4745. Ned Tijdschr Geneeskd. 2012. PMID: 22759710 Dutch.
-
[Diagnosis and treatment of primary hemochromatosis].Ned Tijdschr Geneeskd. 1999 Jul 3;143(27):1404-8. Ned Tijdschr Geneeskd. 1999. PMID: 10422553 Review. Dutch.
-
How we manage patients with hereditary haemochromatosis.Br J Haematol. 2016 Dec;175(5):759-770. doi: 10.1111/bjh.14376. Epub 2016 Oct 10. Br J Haematol. 2016. PMID: 27723100 Review.
Cited by
-
Higher age at diagnosis of hemochromatosis is the strongest predictor of the occurrence of hepatocellular carcinoma in the Swiss hemochromatosis cohort: A prospective longitudinal observational study.Medicine (Baltimore). 2018 Oct;97(42):e12886. doi: 10.1097/MD.0000000000012886. Medicine (Baltimore). 2018. PMID: 30335010 Free PMC article.
-
Patients with hereditary hemochromatosis reach safe range of transferrin saturation sooner with erythrocytaphereses than with phlebotomies.J Clin Apher. 2022 Feb;37(1):100-105. doi: 10.1002/jca.21956. Epub 2021 Dec 13. J Clin Apher. 2022. PMID: 34897777 Free PMC article.
-
European Association for Study of the Liver (EASL) clinical practice guidelines on haemochromatosis.Frontline Gastroenterol. 2023 Mar 15;14(4):282-286. doi: 10.1136/flgastro-2022-102296. eCollection 2023. Frontline Gastroenterol. 2023. PMID: 37409332 Free PMC article.
-
Safety and Efficacy of Therapeutic Erythrocytapheresis Treatment in Chronic Mountain Sickness Patients in Shigatse, Tibet, China.Med Sci Monit. 2020 Dec 23;26:e927853. doi: 10.12659/MSM.927853. Med Sci Monit. 2020. PMID: 33353927 Free PMC article. Clinical Trial.
-
Nrf2 activators for the treatment of rare iron overload diseases: From bench to bedside.Redox Biol. 2025 Apr;81:103551. doi: 10.1016/j.redox.2025.103551. Epub 2025 Feb 14. Redox Biol. 2025. PMID: 39965404 Free PMC article. Review.
References
-
- Asberg A, Hveem K, Thorstensen K, et al. Screening for hemochromatosis: high prevalence and low morbidity in an unselected population of 65,238 persons. Scand J Gastroenterol. 2001;36:1108–15. - PubMed
-
- Adams PC, Barton JC. Haemochromatosis. Lancet. 2007;370:1855–60. - PubMed
-
- Yen AW, Fancher TL, Bowlus CL. Revisiting hereditary hemochromatosis: current concepts and progress. Am J Med. 2006;119:391–9. - PubMed
-
- Adams PC, Reboussin DM, Barton JC, et al. Hemochromatosis and iron-overload screening in a racially diverse population. N Engl J Med. 2005;352:1769–78. - PubMed
-
- Brittenham GM. Disorders of iron metabolism: Iron deficiency and iron overload. In: Hoffman R, Benz EJ, Shattil SJ, Furie B, Silberstein LE, McGlave P, et al., editors. Hematology: Basic Principles and Practice. Philadelphia: Churchill Livingstone Elsevier; 2008. pp. 453–68.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
