

Review
doi: 10.1102/1470-7330.2013.0036.
Imaging of musculoskeletal lymphoma
Affiliations
- PMID: 24334414
- PMCID: PMC3864222
- DOI: 10.1102/1470-7330.2013.0036
Item in Clipboard
Review
Imaging of musculoskeletal lymphoma
Cancer Imaging.
.
Abstract
Lymphoma of the musculoskeletal system involving the bone, muscle or skin is commonly due to secondary involvement from disseminated disease but can occasionally present as primary extranodal disease. Although radiological features are traditionally known to be non-specific, recognition of certain characteristics using summation of imaging modalities as well as knowledge of clinical features can help in making the diagnosis. Imaging also plays an integral role in treatment response assessments, especially via positron emission tomography/computed tomography functional imaging.
Figures
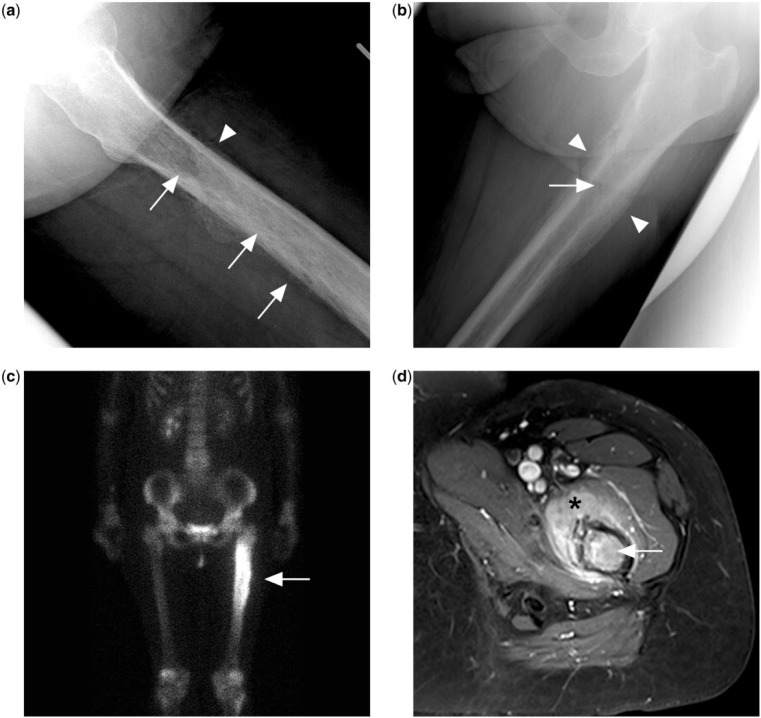
(a) Permeative lytic lesion in the proximal femur diaphysis (arrows) on the lateral left hip radiograph of a patient presenting with left hip pain. There is also a suggestion of irregular periosteal reaction (arrowhead). (b) Dedicated femur radiograph better shows a laminated peristeal reaction (arrowheads) but the permeative lytic lesion is more subtle (arrow). (c) Bone scan with technetium-99m methylene diphosphonate shows intense tracer uptake at the corresponding area. (d) Contrast-enhanced T1-weighted fat-saturated MR image showing marrow enhancement in the femur (arrow) and surrounding enhancing extra-osseous soft tissue mass (black asterisk). Biopsy subsequently confirmed a diagnosis of PBL.
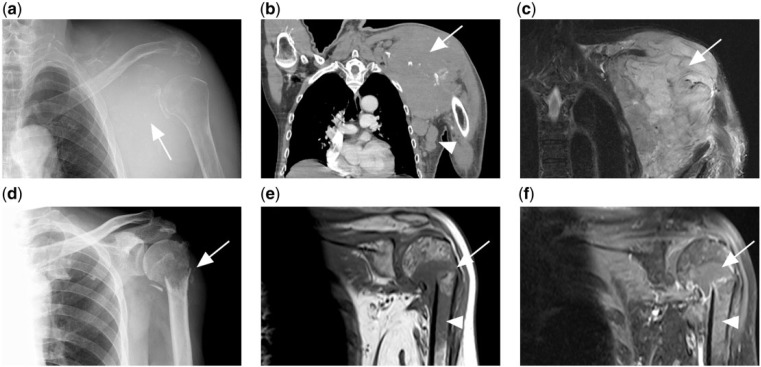
(a) Lytic destruction of the left scapula (white arrow) with soft tissue swelling in a patient with disseminated diffuse large B-cell lymphoma (DLBCL). (b) CT and (c) T2-weighted fat-saturated MR image of same patient showing the tumour mass (arrow). Associated axillary lymphadenopathy is also present (white arrowhead). (d) Another patient with disseminated DLBCL presented with pathological fracture of the left humeral neck. (e) T1-weighted and (f) contrast-enhanced T1-weighted fat-saturated MR images of the same patient showing a T1 hypointense tumour mass at the fracture site, which enhances after contrast (arrow). Marrow involvement of the humeral shaft is also present (arrowhead).
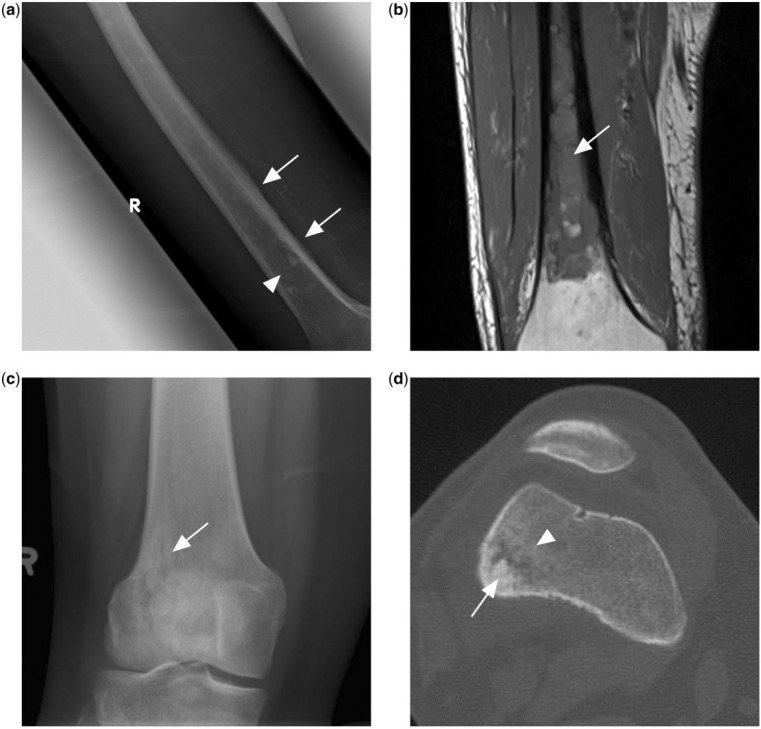
(a) Ill-defined mixed lytic sclerotic lesion in the mid to distal femoral shaft (arrowhead) with adjacent irregular periosteal reaction (arrows). (b) T1-weighted MR image of the same patient showing extensive T1 hypointense marrow changes in the femoral shaft, subsequently found to represent PBL. (c) Knee radiograph of another patient with PBL showing an ill-defined lytic sclerotic lesion (arrow) in the metaphysis of the distal femur. (d) CT scan of the same patient in the bone window shows central sclerotic sequestrum (arrow) with surrounding patchy sclerosis (arrowhead).
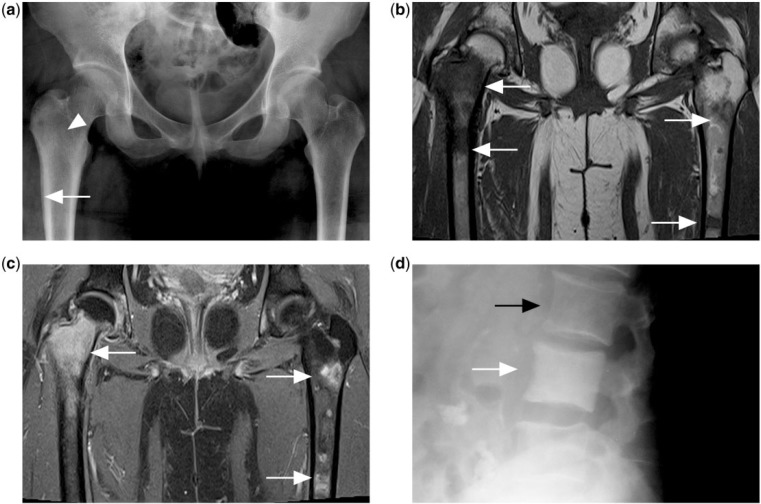
(a) Pelvic radiograph of a patient with disseminated Hodgkin lymphoma showing faint increased sclerosis in the right femur intertrochanteric region (white arrowhead) with layered periosteal reaction in the right proximal femur metadiaphyseal region (white arrow). Note apparent normal appearance of the left proximal femur. (b) T1-weighted and (c) contrast-enhanced T1-weighted fat-saturated MR images showing multiple foci of T1 hypointense and enhancing marrow lesions (white arrows) in both femora. (d) Diffusely increased sclerosis of the vertebral body (white arrow) compared with adjacent normal vertebral body (black arrow) is described as ivory vertebrae in another patient with Hodgkin lymphoma.
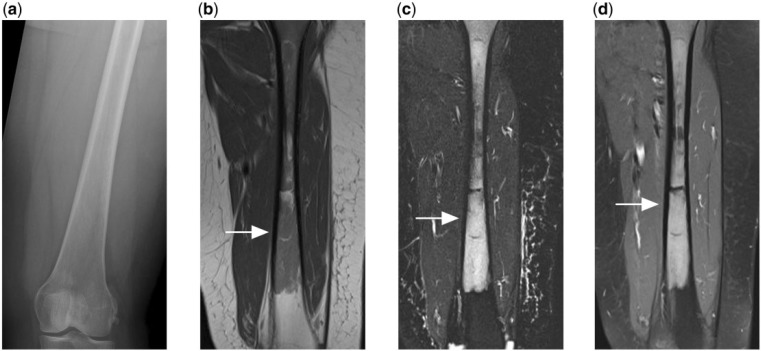
(a) Normal appearing radiograph of the femur of a patient who presented with persistent thigh pain. (b) T1-weighted, (c) T2-weighted fat-saturated and (d) contrast-enhanced T1-weighted fat-saturated MR images reveal florid marrow disease that is T1 hypointense, T2 hyperintense and shows enhancement after contrast. Subsequent biopsy confirmed the diagnosis of PBL.
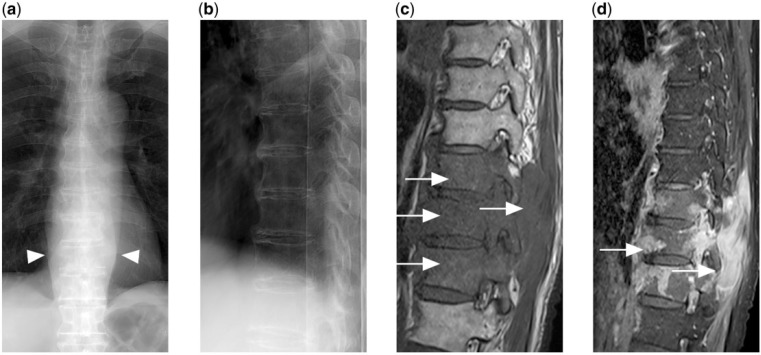
(a) Frontal and (b) lateral radiograph of the thoracic spine shows no obvious fracture or lytic destruction. However, widened paravertebral stripes are present (arrowheads). (c) T1-weighted and (d) contrast-enhanced T1-weighted fat-saturated MR images show extensive enhancing hypointense marrow disease with extra-osseous soft tissue (arrows) in the lower thoracic spine secondary to disseminated DLBCL.
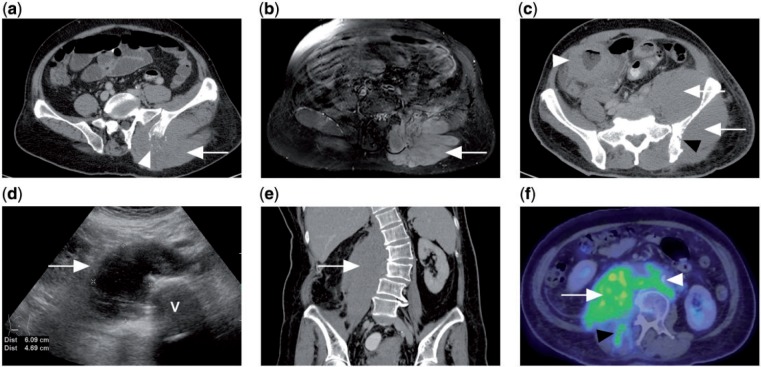
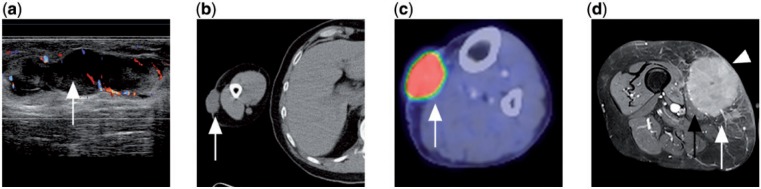
(a) CT of a patient with disseminated DLBCL showing diffuse enlargement of the left gluteus muscle (white arrow) with adjacent lytic destruction of the left iliac bone (white arrowhead). (b) Contrast-enhanced T1-weighted fat-saturated MR image of the same patient showing diffusely enlarged and enhancing left gluteus and erector spinae muscles. (c) CT of a different patient with Burkitt lymphoma of the colon (white arrowhead). There is diffuse involvement of the left gluteus and iliacus muscles (white arrows) with erosion of underlying iliac bone (black arrowhead). (d) Ultrasonograph of the abdomen of another patient with abdominal pain shows a hypoechoic right paravertebral mass. V indicates vertebral body. (e) Coronal CT of the same patient shows the ultrasonographic finding to be a diffusely enlarged right psoas muscle, subsequently diagnosed as marginal zone lymphoma on biopsy. (f) PET/CT with FDG showing avidity of the tumour (white arrow), which extends to the right erector spinae muscle (black arrowhead) as well as retroperitoneal lymphadenopathy (white arrowhead).
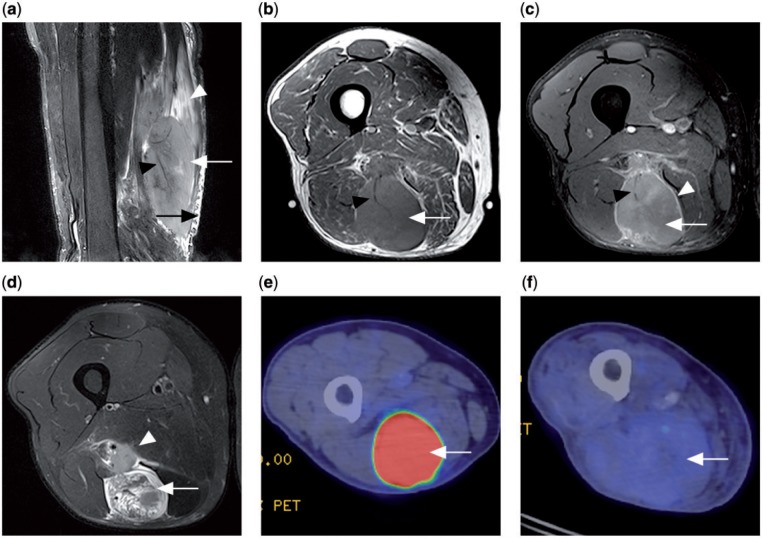
Patient with a primary lymphoma in the semitendinosus muscle. (a) Sagittal T2-weighted fat-saturated MR image showing a T2 hyperintense tumour mass within the muscle (white arrow), long segmental involvement with orientation of the tumour along muscle fascicles (white arrowhead), traversing vessels within involved muscle (black arrowhead) and adjacent subcutaneous stranding (black arrow). (b) Axial T1 MR image showing a tumour of slightly increased signal intensity (white arrow) compared with normal muscles and a traversing vessel (black arrowhead). (c) Contrast-enhanced T1-weighted fat-saturated MR image (white arrow) with peripheral septal enhancement (white arrowhead). Traversing vessel noted again (black arrowhead). (d) Axial T2-weighted fat-saturated MR image showing a heterogeneous T2 hyperintense tumour (white arrow) and adjacent neurovascular bundle involvement (white arrowhead). (e) Prechemotherapy PET/CT with FDG shows the tumour to be FDG avid (white arrow). (f) Postchemotherapy PET/CT showing decrease in FDG avidity of the tumour (white arrow), compatible with treatment response.
(a) Ultrasonograph of a patient with mycosis fungoides showing a dermal lobulated hypoechoic mass with internal vascularity (white arrow). (b) CT of the same patient demonstrates the cutaneous soft tissue mass in the right arm (white arrow). (c) PET/CT with FDG of another patient with mycosis fungoides in the left calf showing an FDG-avid cutaneous soft tissue mass (white arrow). (d) Contrast-enhanced T1-weighted fat-saturated MR image of a different patient with disseminated DLBCL showing an enhancing subcutaneous tumour mass in the medial thigh (white arrow) invading into the skin (white arrowhead) and adjacent sartorius muscle (black arrow).
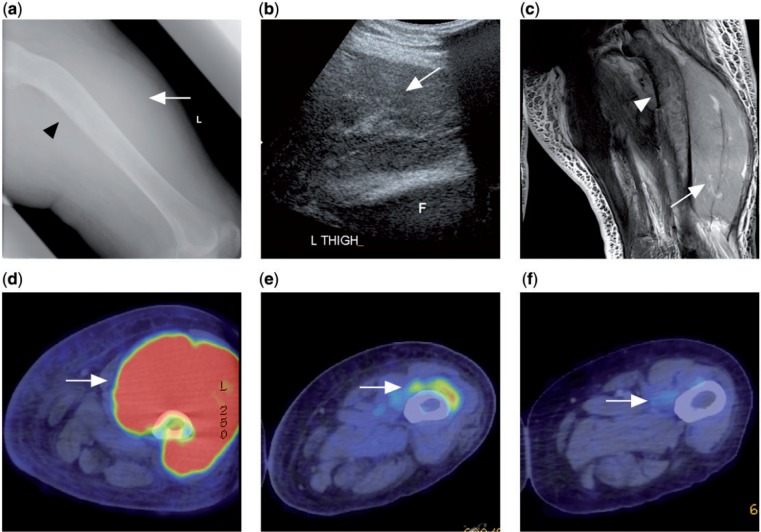
A patient with disseminated follicular lymphoma presented with left thigh swelling. (a) Radiograph of the left femur showing soft tissue swelling in the left thigh (white arrow) with sclerosis and bowing of the left femoral shaft (black arrowhead). (b) Ultrasonograph of the left thigh showing a large heterogeneous swelling of the left quadriceps muscle. F indicates femur. (c) T2-weighted fat-saturated image showing swelling with diffusely raised signal intensity of the quadriceps muscle (white arrow). Marrow involvement of the underlying femur (white arrowhead) also noted. (d) Prechemotherapy PET/CT with FDG showing FDG avidity of the tumour mass. (e, f) Interval PET/CT after chemotherapy showing progressive decrease in size and FDG avidity of the tumour compatible with treatment response (white arrow).
Similar articles
-
Imaging findings of skeletal muscle lymphoma.Clin Imaging. 2014 Sep-Oct;38(5):594-8. doi: 10.1016/j.clinimag.2014.03.006. Epub 2014 Mar 22. Clin Imaging. 2014. PMID: 24735681 Review.
-
Advances in musculoskeletal tumor imaging.Orthop Clin North Am. 2006 Jul;37(3):375-91, vii. doi: 10.1016/j.ocl.2006.05.003. Orthop Clin North Am. 2006. PMID: 16846768 Review.
-
Imaging of lymphoma of the musculoskeletal system.Radiol Clin North Am. 2008 Mar;46(2):379-96, x. doi: 10.1016/j.rcl.2008.03.008. Radiol Clin North Am. 2008. PMID: 18619386 Review.
-
Musculoskeletal neoplasia: helping the orthopaedic surgeon establish the diagnosis.Semin Musculoskelet Radiol. 2007 Mar;11(1):3-15. doi: 10.1055/s-2007-984411. Semin Musculoskelet Radiol. 2007. PMID: 17665346 Review.
-
The evolution of musculoskeletal tumor imaging.Radiol Clin North Am. 2009 May;47(3):435-53. doi: 10.1016/j.rcl.2008.12.002. Radiol Clin North Am. 2009. PMID: 19361669 Review.
Cited by
-
Beneficial effect of consolidative radiotherapy for patients with lymphoma and skeletal involvement.Medicine (Baltimore). 2019 Aug;98(31):e16688. doi: 10.1097/MD.0000000000016688. Medicine (Baltimore). 2019. PMID: 31374054 Free PMC article.
-
Muscular sarcoidosis involving the chest and abdominal walls: case report with MR imaging.Skeletal Radiol. 2018 Mar;47(3):407-411. doi: 10.1007/s00256-017-2787-2. Epub 2017 Oct 16. Skeletal Radiol. 2018. PMID: 29038921
-
Primary lymphoma of bone in children: Three case reports and literature review.Pediatr Discov. 2023 Jun 10;1(1):e15. doi: 10.1002/pdi3.15. eCollection 2023 Jun. Pediatr Discov. 2023. PMID: 40625579 Free PMC article.
-
Primary bone lymphoma: Clinical presentation and therapeutic considerations.J Bone Oncol. 2020 Sep 28;25:100326. doi: 10.1016/j.jbo.2020.100326. eCollection 2020 Dec. J Bone Oncol. 2020. PMID: 33083218 Free PMC article.
-
Preliminary clinical assessment of dynamic carbon-11 methionine positron-emission tomography/computed tomography for the diagnosis of the pathologies in patients with musculoskeletal lesions: a prospective study.Eur J Hybrid Imaging. 2020 Aug 26;4(1):15. doi: 10.1186/s41824-020-00083-x. Eur J Hybrid Imaging. 2020. PMID: 34191157 Free PMC article.
References
-
- Kwee TC, Kwee RM, Nievelstein RA. Imaging in staging of malignant lymphoma: a systematic review. Blood. 2008;15:504–516. - PubMed
-
- Ministry of Health Singapore, National Cancer Registry Interim Annual Registry Report Trends in Cancer Incidence in Singapore 2007–2011. http://www.nrdo.gov.sg/uploadedFiles/NRDO/Cancer_Trends_Report_07–11_for.... Accessed 24th February 2013.
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Ostrowski ML, Unni KK, Banks PM, et al. Malignant Lymphoma of bone. Cancer. 1986;58:2646–2655. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical