

Device-detected atrial fibrillation and risk for stroke: an analysis of >10,000 patients from the SOS AF project (Stroke preventiOn Strategies based on Atrial Fibrillation information from implanted devices)
- PMID: 24334432
- PMCID: PMC3930873
- DOI: 10.1093/eurheartj/eht491
Device-detected atrial fibrillation and risk for stroke: an analysis of >10,000 patients from the SOS AF project (Stroke preventiOn Strategies based on Atrial Fibrillation information from implanted devices)
Abstract
Objective: The aim of this study was to assess the association between maximum daily atrial fibrillation (AF) burden and risk of ischaemic stroke.
Background: Cardiac implanted electronic devices (CIEDs) enhance detection of AF, providing a comprehensive measure of AF burden.
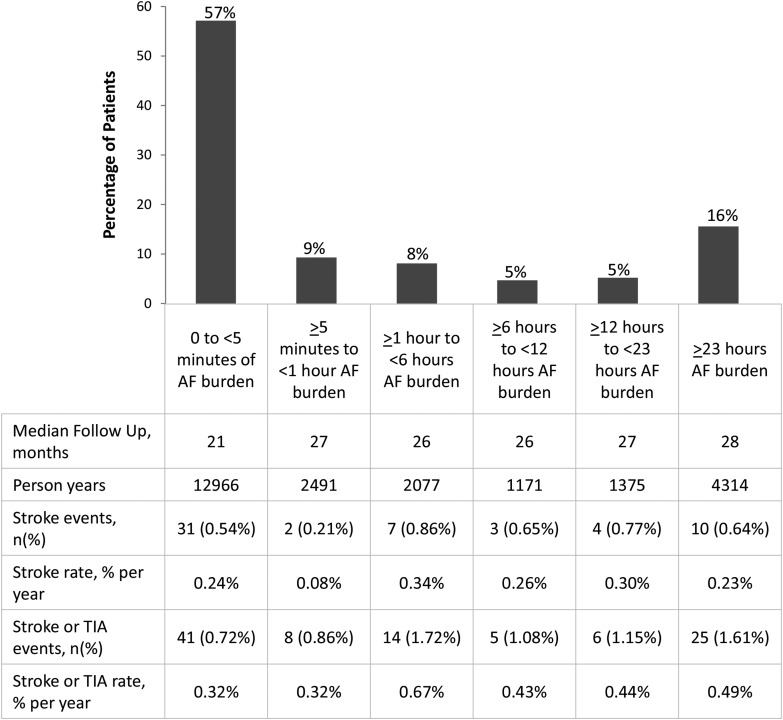
Design, setting, and patients: A pooled analysis of individual patient data from five prospective studies was performed. Patients without permanent AF, previously implanted with CIEDs, were included if they had at least 3 months of follow-up. A total of 10 016 patients (median age 70 years) met these criteria. The risk of ischaemic stroke associated with pre-specified cut-off points of AF burden (5 min, 1, 6, 12, and 23 h, respectively) was assessed.
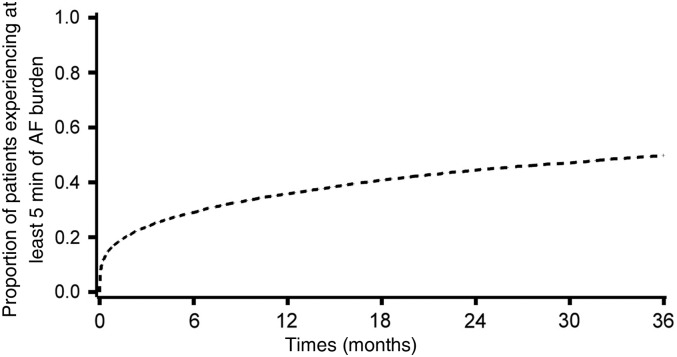
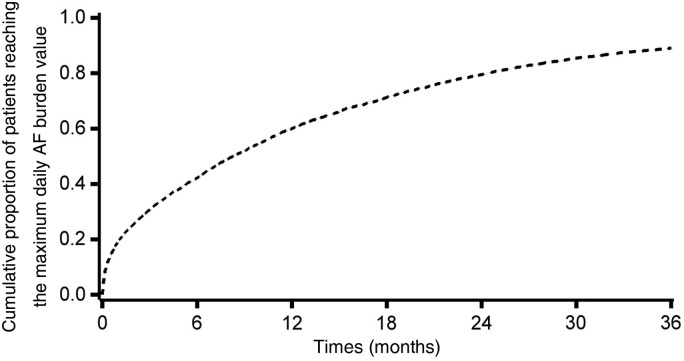
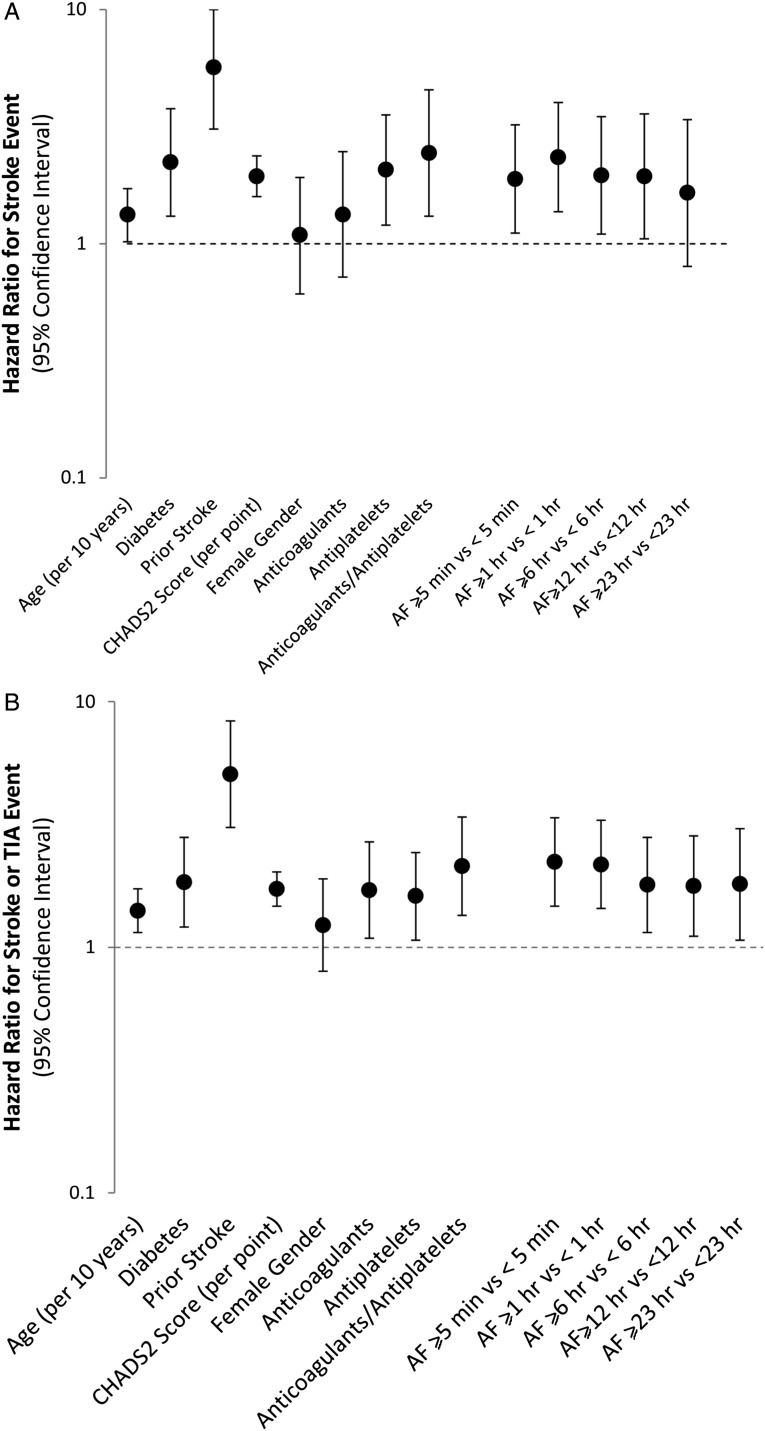
Results: During a median follow-up of 24 months, 43% of 10 016 patients experienced at least 1 day with at least 5 min of AF burden and for them the median time to the maximum AF burden was 6 months (inter-quartile range: 1.3-14). A Cox regression analysis adjusted for the CHADS2 score and anticoagulants at baseline demonstrated that AF burden was an independent predictor of ischaemic stroke. Among the thresholds of AF burden that we evaluated, 1 h was associated with the highest hazard ratio (HR) for ischaemic stroke, i.e. 2.11 (95% CI: 1.22-3.64, P = 0.008).
Conclusions: Device-detected AF burden is associated with an increased risk of ischaemic stroke in a relatively unselected population of CIEDs patients. This finding may add to the basis for timely and clinically appropriate decision-making on anticoagulation treatment.
Keywords: Anticoagulation; Atrial fibrillation; Implantable defibrillator; Pacemaker; Stroke.
Figures
References
-
- Kirchhof P, Lip GY, Van Gelder IC, Bax J, Hylek E, Kaab S, Schotten U, Wegscheider K, Boriani G, Brandes A, Ezekowitz M, Diener H, Haegeli L, Heidbuchel H, Lane D, Mont L, Willems S, Dorian P, Aunes-Jansson M, Blomstrom-Lundqvist C, Borentain M, Breitenstein S, Brueckmann M, Cater N, Clemens A, Dobrev D, Dubner S, Edvardsson NG, Friberg L, Goette A, Gulizia M, Hatala R, Horwood J, Szumowski L, Kappenberger L, Kautzner J, Leute A, Lobban T, Meyer R, Millerhagen J, Morgan J, Muenzel F, Nabauer M, Baertels C, Oeff M, Paar D, Polifka J, Ravens U, Rosin L, Stegink W, Steinbeck G, Vardas P, Vincent A, Walter M, Breithardt G, Camm AJ. Comprehensive risk reduction in patients with atrial fibrillation: emerging diagnostic and therapeutic options—a report from the 3rd Atrial Fibrillation Competence NETwork/European Heart Rhythm Association consensus conference. Europace. 2012;14:8–27. - PMC - PubMed
-
- Camm AJ, Corbucci G, Padeletti L. Usefulness of continuous electrocardiographic monitoring for atrial fibrillation. Am J Cardiol. 2012;110:270–276. - PubMed
-
- Glotzer TV, Hellkamp AS, Zimmerman J, Sweeney MO, Yee R, Marinchak R, Cook J, Paraschos A, Love J, Radoslovich G, Lee KL, Lamas GA. Atrial high rate episodes detected by pacemaker diagnostics predicts death and stroke. Circulation. 2003;107:1614–1619. - PubMed
-
- Capucci A, Santini M, Padeletti L, Gulizia M, Botto G, Boriani G, Ricci R, Favale S, Zolezzi F, Di Belardino N, Molon G, Drago F, Villani GQ, Mazzini E, Vimercati M, Grammatico A. Monitored atrial fibrillation duration predicts arterial embolic events in patients suffering from bradycardia and atrial fibrillation implanted with antitachycardia pacemakers. J Am Coll Cardiol. 2005;46:1913–1920. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
