

Malignant abdominal rocks: where do they come from?
- PMID: 24334568
- PMCID: PMC3864229
- DOI: 10.1102/1470-7330.2013.0048
Malignant abdominal rocks: where do they come from?
Abstract
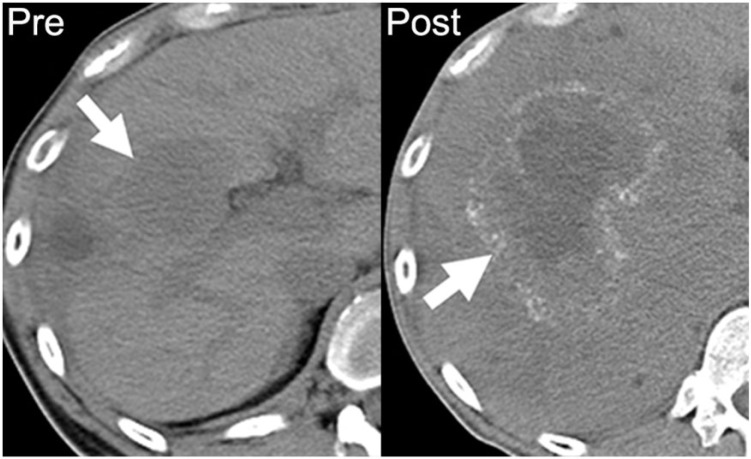
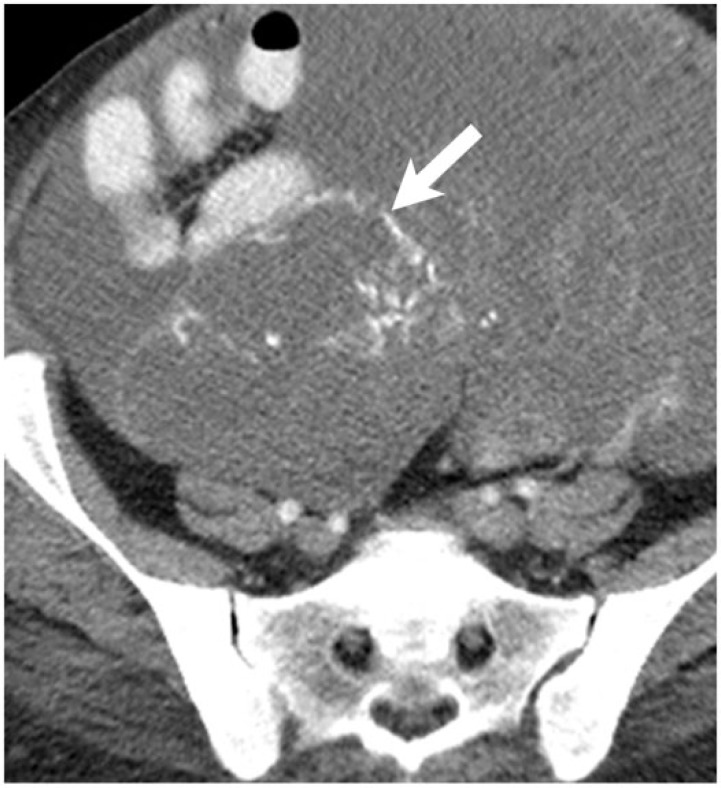
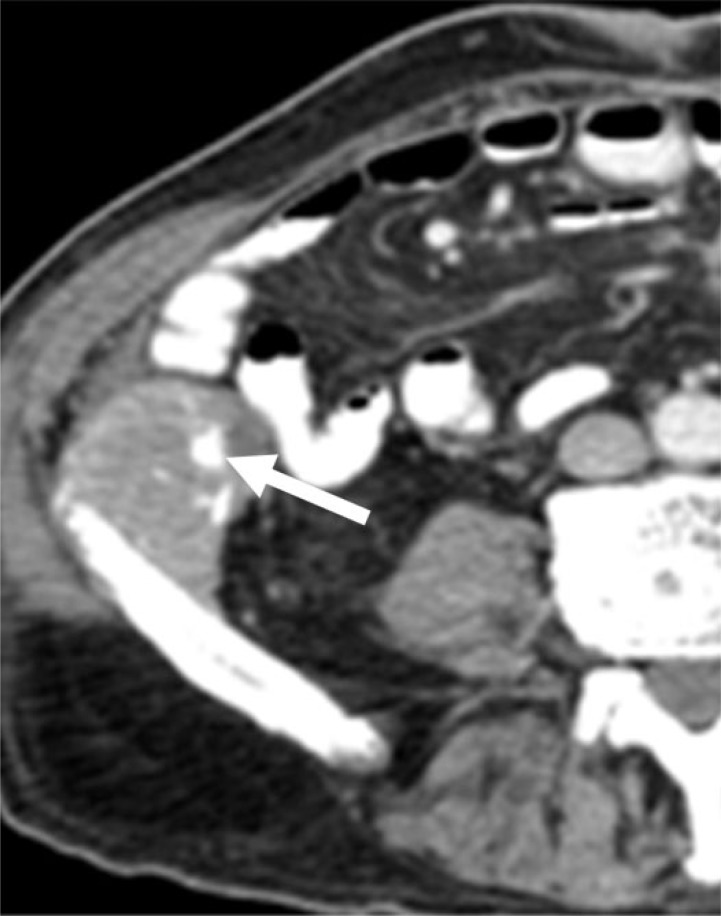
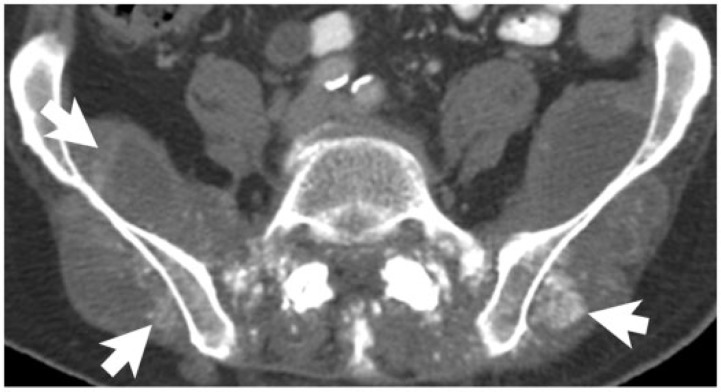
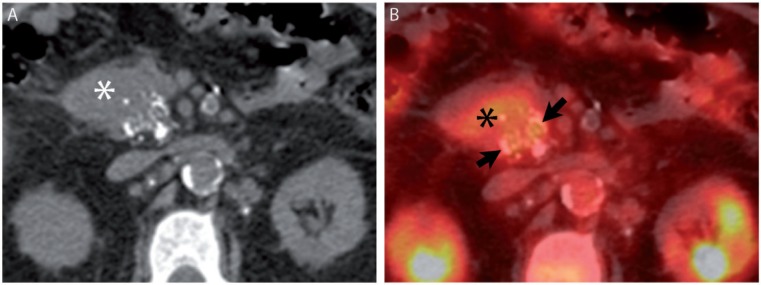
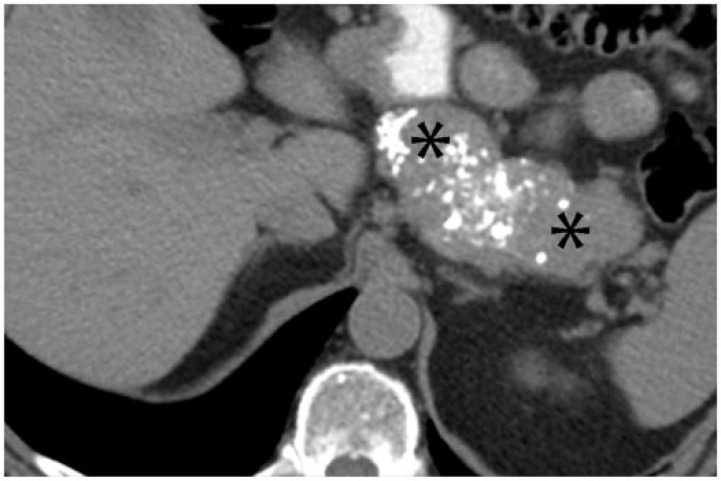
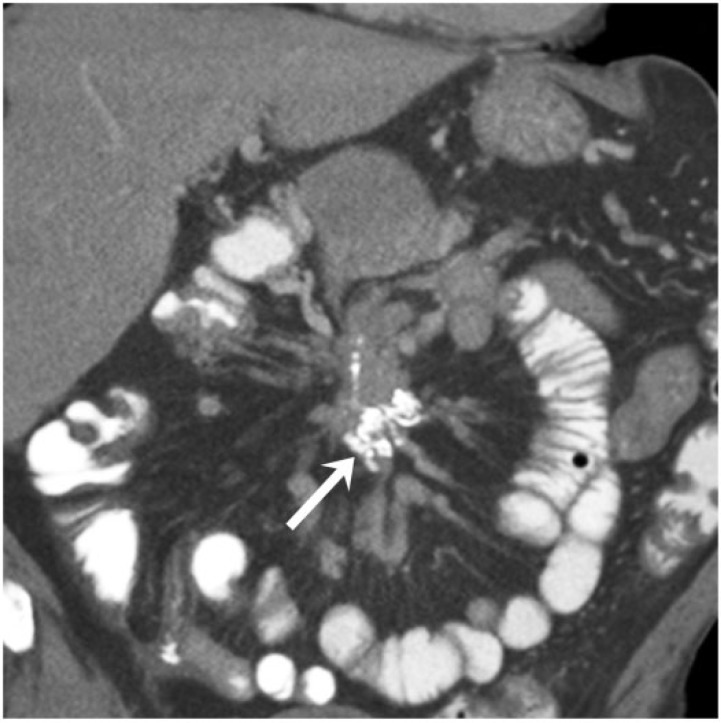
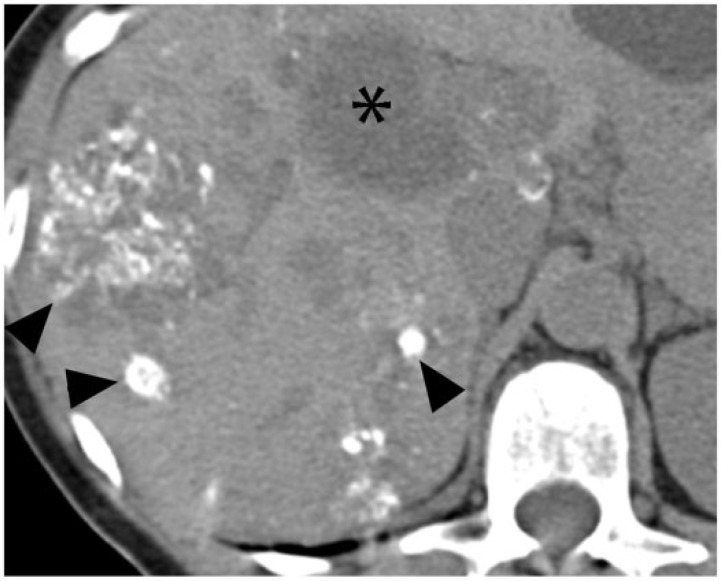
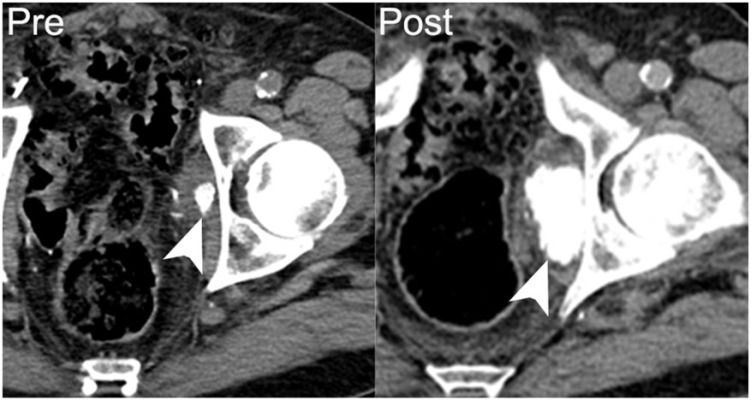
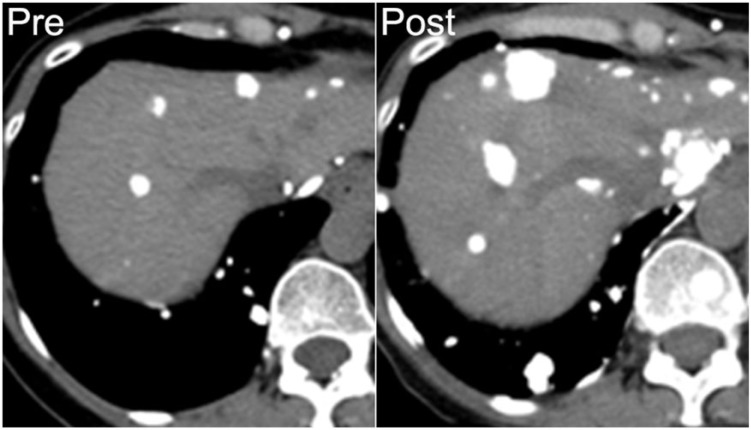
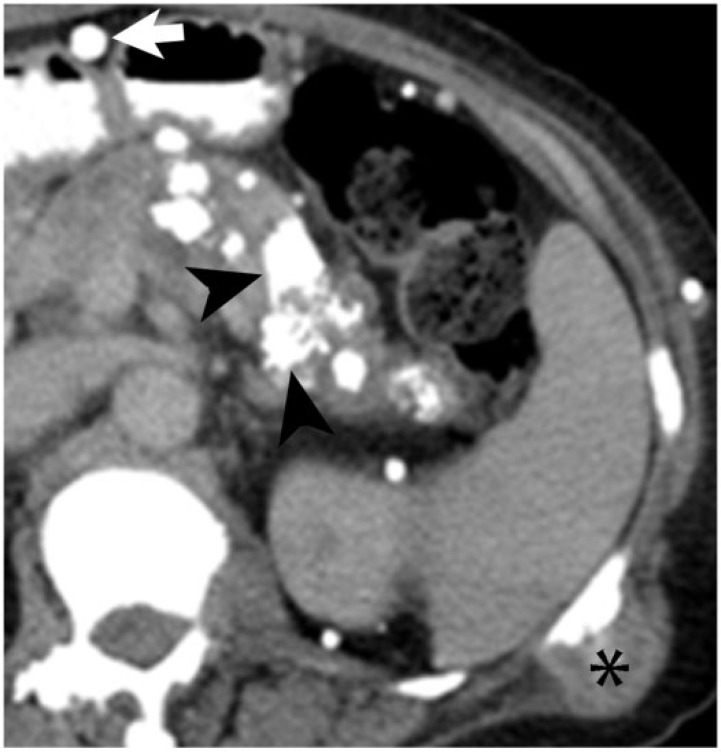
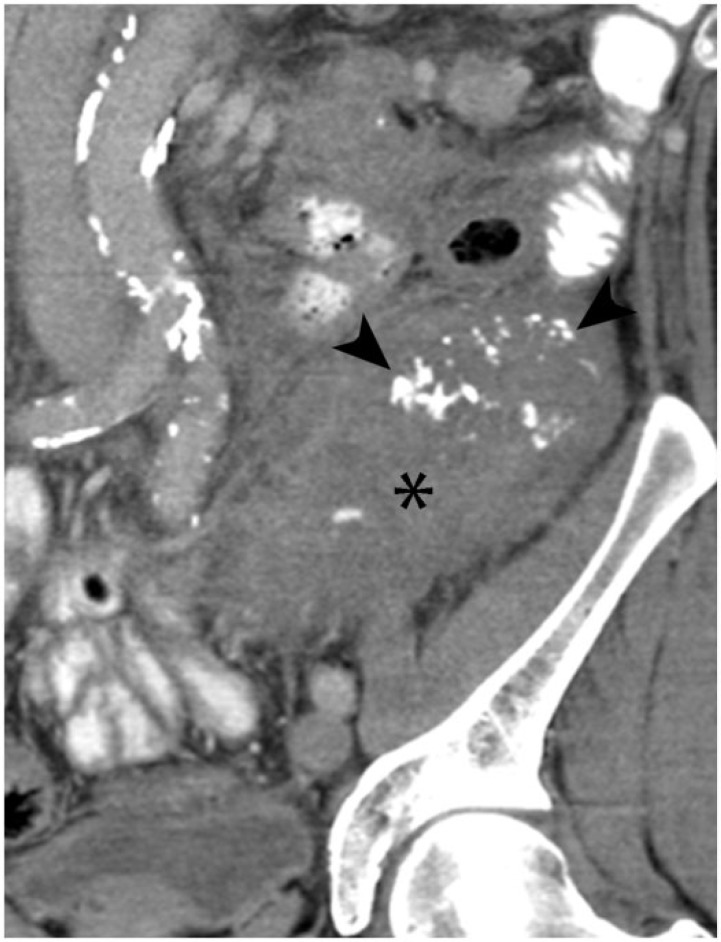
For the radiologist, calcifications in an abdominal malignancy raise questions of both diagnostic and prognostic significance. Although certain cancers are well known to calcify, such as colorectal and ovarian, malignant abdominal calcifications actually arise from a wide variety of epithelial, mesenchymal, lymphoid, or germ cell neoplasms. The pathophysiology of calcification in abdominal malignancies is heterogeneous and incompletely understood. Calcifications may present primarily, in untreated tumors, or develop during treatment; the latter can occur in variable clinical settings. A basic understanding of the varied pathogenic etiology can assist the radiologist in assessing disease status. By presenting an assortment of calcified abdominal malignancies on computed tomography in varied clinical settings, we aim not only to inform the differential diagnosis, but also to clarify the prognosis of calcifications in abdominal malignancies.
Figures



Similar articles
-
Ovarian malignant germ cell tumors: cellular classification and clinical and imaging features.Radiographics. 2014 May-Jun;34(3):777-801. doi: 10.1148/rg.343130067. Radiographics. 2014. PMID: 24819795 Review.
-
Metachronous Synovial Sarcoma After Treatment of Mixed Germ Cell Tumor in a Child with Complete Gonadal Dysgenesis.J Clin Res Pediatr Endocrinol. 2018 Mar 1;10(1):87-90. doi: 10.4274/jcrpe.4905. Epub 2017 Aug 24. J Clin Res Pediatr Endocrinol. 2018. PMID: 28836496 Free PMC article.
-
Ovarian tumours in childhood and adolescence.Eur J Gynaecol Oncol. 2010;31(6):616-20. Eur J Gynaecol Oncol. 2010. PMID: 21319502 Review.
-
[Malignant germ cell tumors in children or malignant teratomas].Arch Fr Pediatr. 1983 Feb;40(2):117-22. Arch Fr Pediatr. 1983. PMID: 6307207 French. No abstract available.
-
[Serous cystadenocarcinoma of the ovary: unusual visualization of calcified intraperitoneal metastases in CT and bone scintigraphy].Rontgenblatter. 1987 Aug;40(8):260-2. Rontgenblatter. 1987. PMID: 3629146 German.
Cited by
-
Superior mesenteric vein tumour thrombus in a patient with caecal adenocarcinoma: a rare and important finding.BJR Case Rep. 2021 Jan 5;7(2):20200147. doi: 10.1259/bjrcr.20200147. eCollection 2021 Apr 1. BJR Case Rep. 2021. PMID: 33841906 Free PMC article.
-
The CT scout view: complementary value added to abdominal CT interpretation.Abdom Radiol (NY). 2021 Oct;46(10):5021-5036. doi: 10.1007/s00261-021-03135-3. Epub 2021 Jun 1. Abdom Radiol (NY). 2021. PMID: 34075469 Review.
-
Calcifications and Cystic Morphology on Preoperative Imaging Predict Survival After Resection of Pancreatic Neuroendocrine Tumors.Ann Surg Oncol. 2023 Apr;30(4):2424-2430. doi: 10.1245/s10434-022-12783-8. Epub 2022 Nov 25. Ann Surg Oncol. 2023. PMID: 36434481
-
Primary extraskeletal osteosarcoma of small bowel mesentery presenting with acute bowel obstruction.J Radiol Case Rep. 2021 Dec 1;15(12):10-19. doi: 10.3941/jrcr.v15i12.4329. eCollection 2021 Dec. J Radiol Case Rep. 2021. PMID: 35519001 Free PMC article.
-
Increase in post-therapy tumor calcification on CT scan is not an indicator of response to therapy in low-grade serous ovarian cancer.Abdom Radiol (NY). 2016 Aug;41(8):1589-95. doi: 10.1007/s00261-016-0701-3. Abdom Radiol (NY). 2016. PMID: 26969496 Free PMC article.
References
-
- Porth CM. Essentials of pathophysiology: concepts of altered health states. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010.
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA-A Cancer J Clin. 2013;63:11–30. - PubMed
-
- Agarwal A, Yeh BM, Breiman BM, Qayyum A, Coakley FV. Peritoneal calcification: causes and distinguishing features on CT. Am J Roentgenol. 2004;182:441–445. - PubMed
-
- Scatarige JC, Fishman EK, Saksouk FA, Siegelman SS. Computed tomography of calcified liver masses. J Comput Assisted Tomogr. 1983;7:83–89. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources