

A mathematical model to evaluate the routine use of fecal microbiota transplantation to prevent incident and recurrent Clostridium difficile infection
- PMID: 24334794
- PMCID: PMC3977703
- DOI: 10.1086/674394
A mathematical model to evaluate the routine use of fecal microbiota transplantation to prevent incident and recurrent Clostridium difficile infection
Abstract
Objective: Fecal microbiota transplantation (FMT) has been suggested as a new treatment to manage Clostridium difficile infection (CDI). With use of a mathematical model of C. difficile within an intensive care unit (ICU), we examined the potential impact of routine FMT.
Design, setting, and patients: A mathematical model of C. difficile transmission, supplemented with prospective cohort, surveillance, and billing data from hospitals in the southeastern United States.
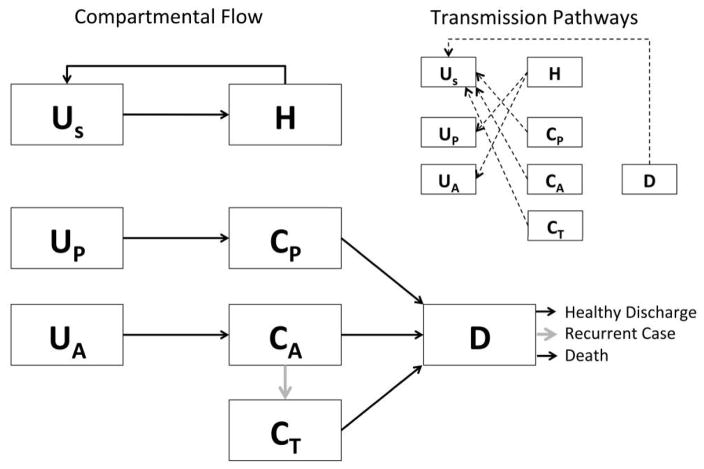
Methods: Cohort, surveillance, and billing data as well as data from the literature were used to construct a compartmental model of CDI within an ICU. Patients were defined as being in 1 of 6 potential health states: uncolonized and at low risk; uncolonized and at high risk; colonized and at low risk; colonized and at high risk; having CDI; or treated with FMT.
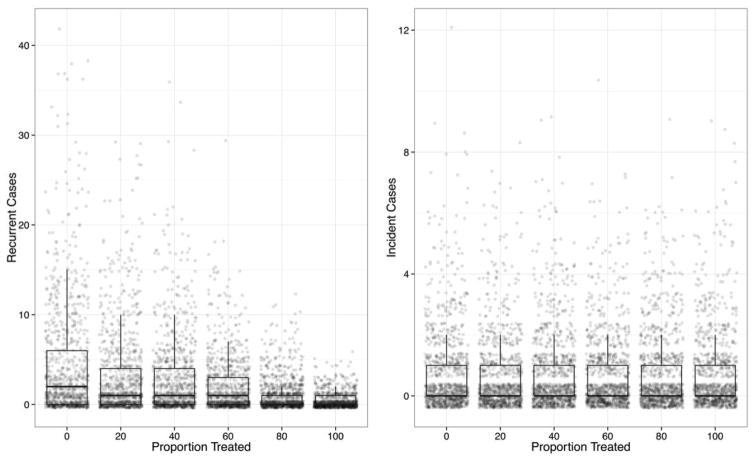
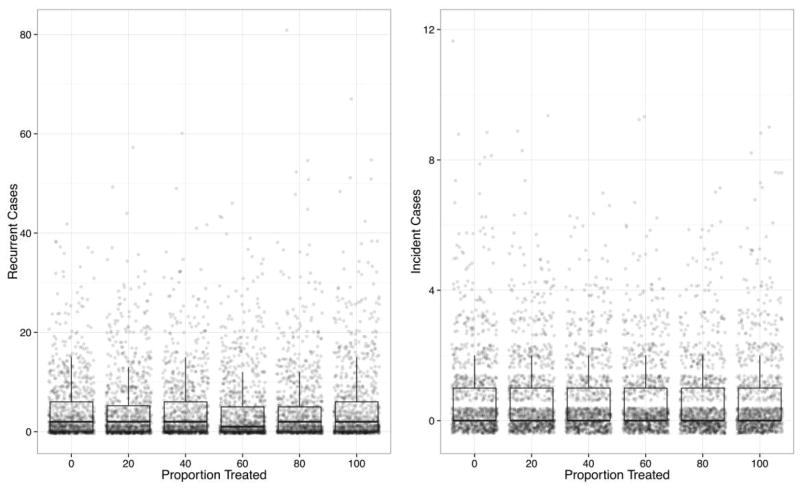
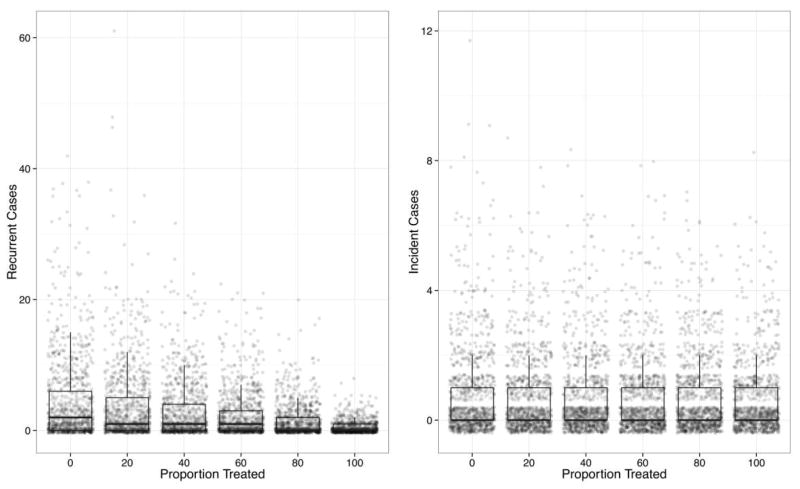
Results: The use of FMT to treat patients after CDI was associated with a statistically significant reduction in recurrence but not with a reduction in incident cases. Treatment after administration of high-risk medications, such as antibiotics, did not result in a decrease in recurrence but did result in a statistically significant difference in incident cases across treatment groups, although whether this difference was clinically relevant was questionable.
Conclusions: Our study is a novel mathematical model that examines the effect of FMT on the prevention of recurrent and incident CDI. The routine use of FMT represents a promising approach to reduce complex recurrent cases, but a reduction in CDI incidence will require the use of other methods to prevent transmission.
Conflict of interest statement
Figures
Comment in
-
Fecal microbiota therapy: ready for prime time?Infect Control Hosp Epidemiol. 2014 Jan;35(1):28-30. doi: 10.1086/674395. Epub 2013 Dec 2. Infect Control Hosp Epidemiol. 2014. PMID: 24334795 Free PMC article. No abstract available.
References
-
- Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA) Infect Control Hosp Epidemiol. 2010;31(5):431–455. - PubMed
-
- Kwok CS, Arthur AK, Anibueze CI, Singh S, Cavallazzi R, Loke YK. Risk of Clostridium difficile infection with acid suppressing drugs and antibiotics: meta-analysis. Am J Gastroenterol. 2012;107(7):1011–1019. - PubMed
-
- Garey KW, Sethi S, Yadav Y, DuPont HL. Meta-analysis to assess risk factors for recurrent Clostridium difficile infection. J Hosp Infect. 2008;70(4):298–304. - PubMed
-
- Agency for Healthcare Research and Quality. HCUPnet; 2006. [Accessed September 17, 2012]. http://hcupnet.ahrq.gov/
-
- Miller BA, Chen LF, Sexton DJ, Anderson DJ. Comparison of the burdens of hospital-onset, healthcare facility-associated Clostridium difficile infection and of healthcare–associated infection due to methicillin-resistant Staphylococcus aureus in community hospitals. Infect Control Hosp Epidemiol. 2011;32(4):387–390. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical