

Review
doi: 10.1161/JAHA.113.000536.
The cGMP signaling pathway as a therapeutic target in heart failure with preserved ejection fraction
Affiliations
- PMID: 24334823
- PMCID: PMC3886746
- DOI: 10.1161/JAHA.113.000536
Item in Clipboard
Review
The cGMP signaling pathway as a therapeutic target in heart failure with preserved ejection fraction
J Am Heart Assoc.
.
No abstract available
Keywords: cGMP; heart failure; phosphodiesterase 5; preserved ejection fraction; soluble guanylate cyclase.
Figures
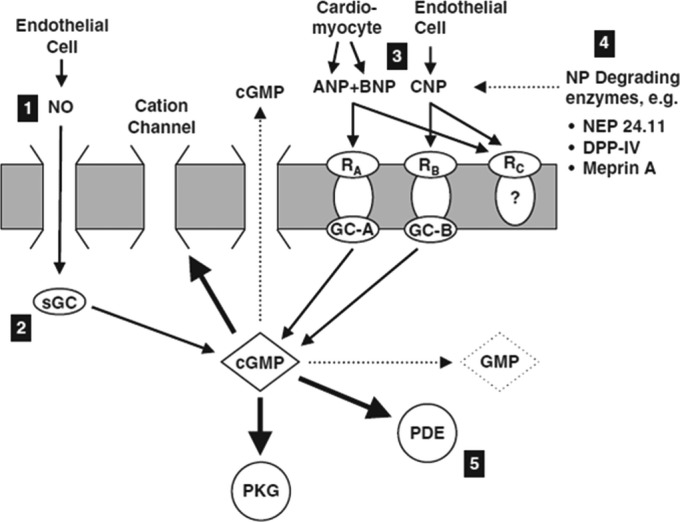
cGMP signaling pathways. cGMP is the second messenger of 2 distinct signaling pathways: (1) NO is produced by endothelial cells and binds to sGC in the target cell; and (2) ANP and BNP, derived primarily from cardiomyocytes, stimulate GC‐A, whereas CNP, secreted by endothelial cells, stimulates GC‐B. cGMP signaling may be augmented by (1) the use of NO mimetics such as nitrovasodilators; (2) sGC activators or stimulators; (3) increasing levels of natriuretic peptides; (4) by inhibiting natriuretic peptide degrading enzymes; and (5) inhibiting the activity of cGMP‐hydrolyzing PDEs. ANP indicates atrial natriuretic peptide; BNP, B‐type natriuretic peptide; cGMP, cyclic guanosine monophosphate; CNP, C‐type natriuretic peptide; DPP4, dipeptidyl peptidase IV; GC, guanylate cyclase; GMP, guanosine monophosphate; NEP, neutral endopeptidase; NO, nitric oxide; PDE, phosphodiesterase; PKG, protein kinase G; RA, natriuretic peptide receptor A; sGC, soluble guanylate cyclase. Adapted with permission from Boerrigter et al.

cGMP signaling and myocardial dysfunction and remodeling in HFpEF. Comorbidities induce a systemic proinflammatory state with elevated plasma levels of interleukin (IL)–6, tumor necrosis factor (TNF)–α, soluble ST2 (sST2), and pentraxin 3. Coronary microvascular endothelial cells reactively produce reactive oxygen species (ROS), vascular cell adhesion molecules (VCAMs), and E‐selectin. Production of ROS leads to formation of peroxynitrite (ONOO−) and reduced nitric oxide (NO) bioavailability, both of which lower soluble guanylate cyclase (sGC) activity in adjacent cardiomyocytes. Lower sGC activity decreases cyclic guanosine monophosphate concentration and protein kinase G (PKG) activity. Low PKG activity increases resting tension (Fpassive) of cardiomyocytes because of hypophosphorylation of titin and removes the brake on prohypertrophic stimuli inducing cardiomyocyte hypertrophy. VCAM and E‐selectin expression in endothelial cells favors migration into the subendothelium of monocytes. These monocytes release transforming growth factor β (TGF‐β). The latter stimulates conversion of fibroblasts to myofibroblasts, which deposit collagen in the interstitial space. cGMP indicates cyclic guanosine monophosphate; COPD, chronic obstructive pulmonary disease; HFpEF, heart failure with preserved ejection fraction. Adapted and modified with permission from Paulus and Tschope.

PKG activity and cGMP concentration in myocardial tissue from patients with heart failure with reduced and preserved ejection fraction and aortic stenosis. AS indicates aortic stenosis; cGMP, cyclic guanosine monophosphate; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; PKG, protein kinase G. Adapted and modified with permission from van Heerebeek et al.

Schematic representation of the mechanism(s) by which NO‐independent sGC stimulators and sGC activators fit into the NO/sGC/cGMP pathway. Oxidative stress—a risk factor for several cardiovascular diseases—is associated with increased formation of reactive oxygen species that are known to oxidize and inactivate many biomolecules, culminating in tissue damage. In particular, ONOO− oxidizes sGC, resulting in loss of the heme group. Heme‐free sGC is unable to respond to NO and can be regarded as a dysfunctional form of the enzyme (NO stimulates only the native form of sGC). Stimulators of sGC have a dual mode of action: they directly stimulate the native form of the enzyme and make it more sensitive to endogenous NO. Activators of sGC specifically activate dysfunctional or heme‐free sGC. Stimulation of native sGC and activation of heme‐free sGC both lead to increased formation of cGMP, which exerts a profound, multifaceted cytoprotective effect. cGMP indicates cyclic guanosine monophosphate; GMP, guanosine monophosphate; GTP, guanosine triphosphate; NO, nitric oxide; NOS, nitric oxide synthase; ONOO−, peroxynitrite; PDE, phosphodiesterase; sGC, soluble guanylate cyclase. Adapted and modified with permission from Hobbs and Stasch.
Similar articles
-
cGMP Signaling and Modulation in Heart Failure.J Cardiovasc Pharmacol. 2020 May;75(5):385-398. doi: 10.1097/FJC.0000000000000749. J Cardiovasc Pharmacol. 2020. PMID: 31464774 Free PMC article. Review.
-
Multiplicity of Nitric Oxide and Natriuretic Peptide Signaling in Heart Failure.J Cardiovasc Pharmacol. 2020 May;75(5):370-384. doi: 10.1097/FJC.0000000000000724. J Cardiovasc Pharmacol. 2020. PMID: 31498237 Review.
-
Therapeutic Stalemate in Heart Failure With Preserved Ejection Fraction.J Am Heart Assoc. 2021 Jun 15;10(12):e021120. doi: 10.1161/JAHA.121.021120. Epub 2021 May 31. J Am Heart Assoc. 2021. PMID: 34056916 Free PMC article. Review.
-
Novel sGC Stimulators and sGC Activators for the Treatment of Heart Failure.Handb Exp Pharmacol. 2017;243:225-247. doi: 10.1007/164_2016_100. Handb Exp Pharmacol. 2017. PMID: 27900610 Review.
-
Leveraging Signaling Pathways to Treat Heart Failure With Reduced Ejection Fraction.Circ Res. 2019 May 24;124(11):1618-1632. doi: 10.1161/CIRCRESAHA.119.313682. Circ Res. 2019. PMID: 31120818 Free PMC article. Review.
Cited by
-
Inhibitory effect of (pro)renin receptor decoy inhibitor PRO20 on endoplasmic reticulum stress during cardiac remodeling.Front Pharmacol. 2022 Aug 12;13:940365. doi: 10.3389/fphar.2022.940365. eCollection 2022. Front Pharmacol. 2022. PMID: 36034809 Free PMC article.
-
Targeting Cyclic Guanylate Monophosphate in Resistant Hypertension and Heart Failure: Are Sacubitril/Valsartan and Vericiguat Synergistic and Effective in Both Conditions?High Blood Press Cardiovasc Prev. 2021 Nov;28(6):541-545. doi: 10.1007/s40292-021-00489-z. Epub 2021 Nov 9. High Blood Press Cardiovasc Prev. 2021. PMID: 34750764 No abstract available.
-
Drugs' development in acute heart failure: what went wrong?Heart Fail Rev. 2018 Sep;23(5):667-691. doi: 10.1007/s10741-018-9707-y. Heart Fail Rev. 2018. PMID: 29736812 Review.
-
Treatment With Treprostinil and Metformin Normalizes Hyperglycemia and Improves Cardiac Function in Pulmonary Hypertension Associated With Heart Failure With Preserved Ejection Fraction.Arterioscler Thromb Vasc Biol. 2020 Jun;40(6):1543-1558. doi: 10.1161/ATVBAHA.119.313883. Epub 2020 Apr 9. Arterioscler Thromb Vasc Biol. 2020. PMID: 32268788 Free PMC article.
-
Pro-Atrial Natriuretic Peptide: A Novel Guanylyl Cyclase-A Receptor Activator That Goes Beyond Atrial and B-Type Natriuretic Peptides.JACC Heart Fail. 2015 Sep;3(9):715-23. doi: 10.1016/j.jchf.2015.03.015. JACC Heart Fail. 2015. PMID: 26362447 Free PMC article.
References
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006; 355:251-259 - PubMed
-
- Steinberg BA, Zhao X, Heidenreich PA, Peterson ED, Bhatt DL, Cannon CP, Hernandez AF, Fonarow GC. Trends in patients hospitalized with heart failure and preserved left ventricular ejection fraction: prevalence, therapies, and outcomes. Circulation. 2012; 126:65-75 - PubMed
-
- Bhatia RS, Tu JV, Lee DS, Austin PC, Fang J, Haouzi A, Gong Y, Liu PP. Outcome of heart failure with preserved ejection fraction in a population‐based study. N Engl J Med. 2006; 355:260-269 - PubMed
-
- Shah RV, Desai AS, Givertz MM. The effect of renin‐angiotensin system inhibitors on mortality and heart failure hospitalization in patients with heart failure and preserved ejection fraction: a systematic review and meta‐analysis. J Card Fail. 2010; 16:260-267 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
