

Duration of symptoms of respiratory tract infections in children: systematic review
- PMID: 24335668
- PMCID: PMC3898587
- DOI: 10.1136/bmj.f7027
Duration of symptoms of respiratory tract infections in children: systematic review
Erratum in
- BMJ. 2014;347:f7575
Abstract
Objective: To determine the expected duration of symptoms of common respiratory tract infections in children in primary and emergency care.
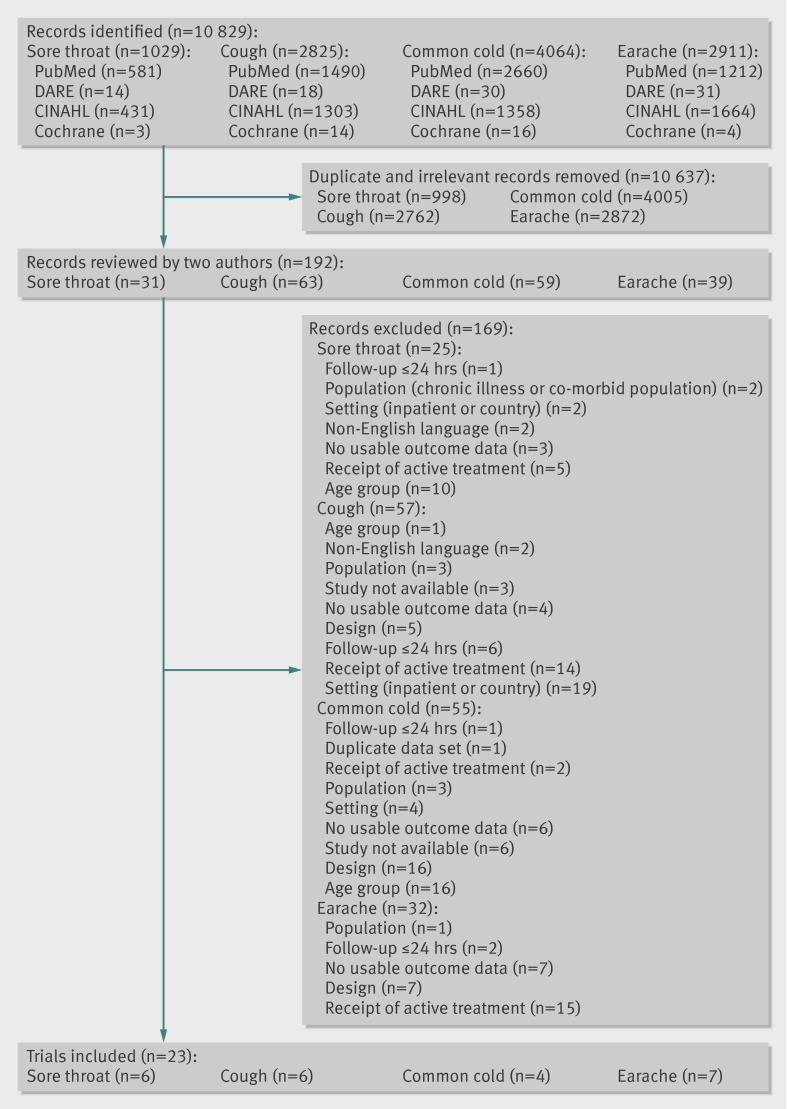
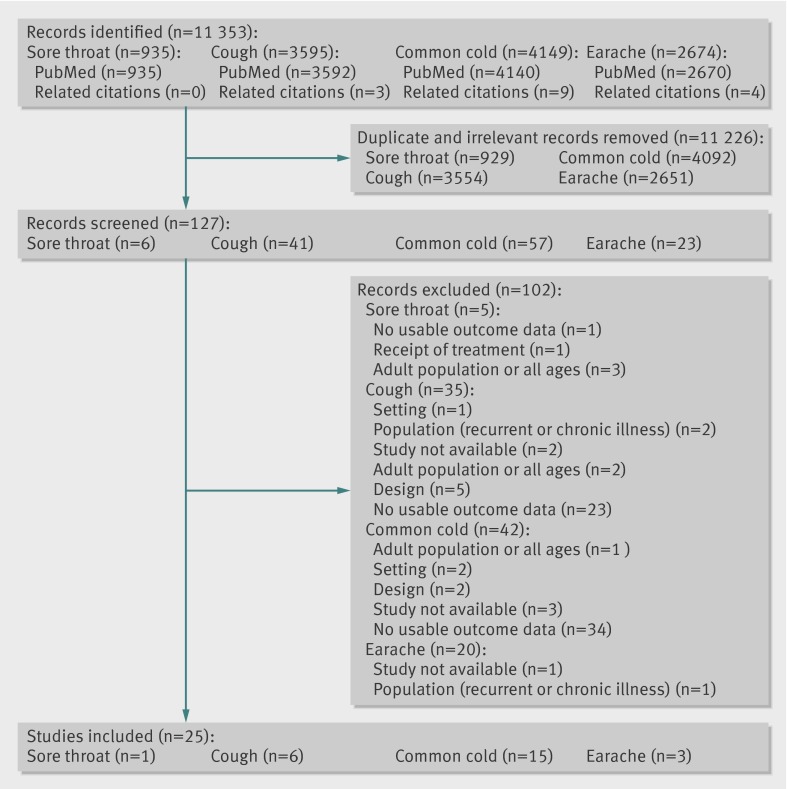
Design: Systematic review of existing literature to determine durations of symptoms of earache, sore throat, cough (including acute cough, bronchiolitis, and croup), and common cold in children.
Data sources: PubMed, DARE, and CINAHL (all to July 2012).
Eligibility criteria for selecting studies: Randomised controlled trials or observational studies of children with acute respiratory tract infections in primary care or emergency settings in high income countries who received either a control treatment or a placebo or over-the-counter treatment. Study quality was assessed with the Cochrane risk of bias framework for randomised controlled trials, and the critical appraisal skills programme framework for observational studies.
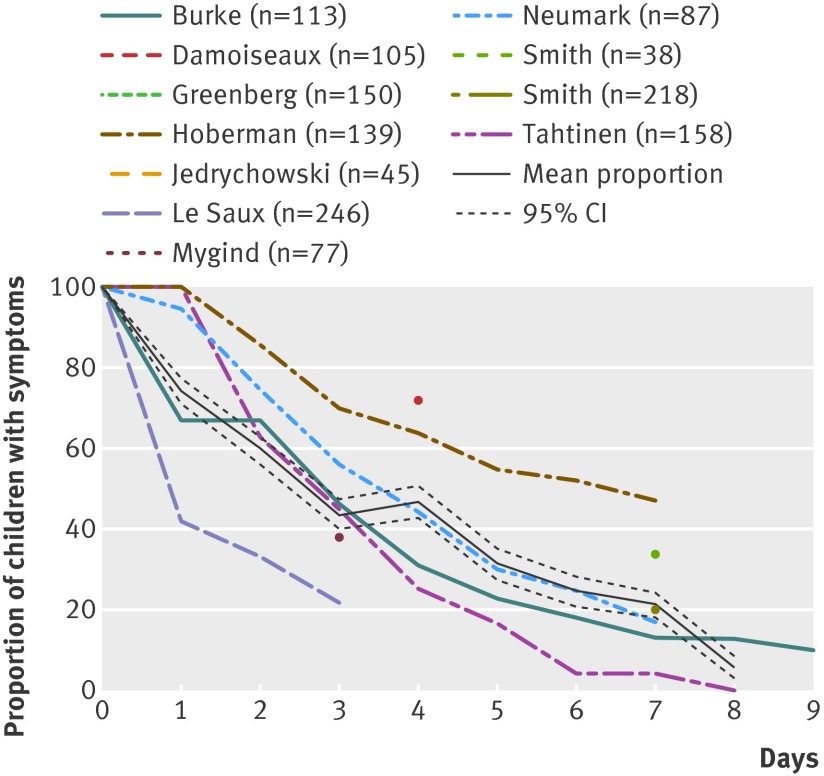
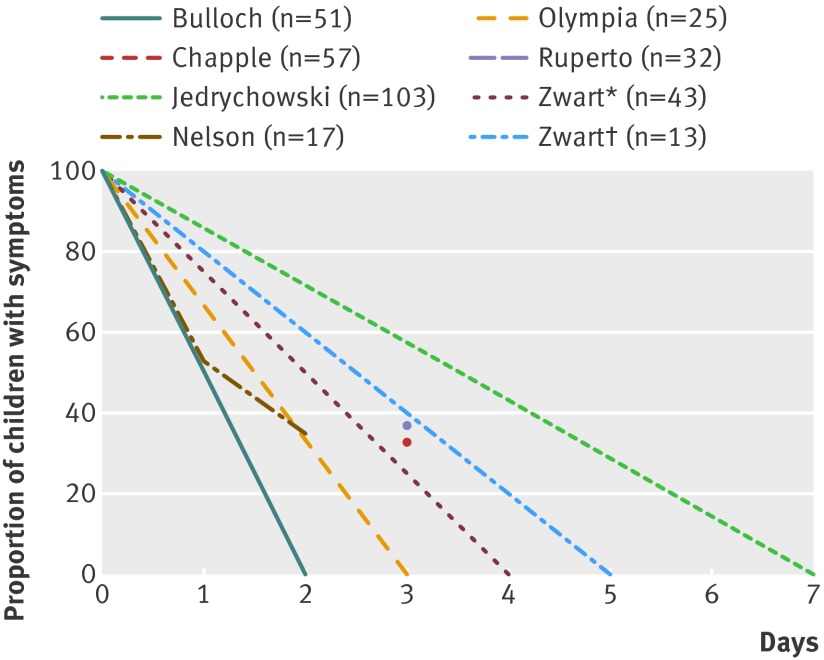
Main outcome measures: Individual study data and, when possible, pooled daily mean proportions and 95% confidence intervals for symptom duration. Symptom duration (in days) at which each symptom had resolved in 50% and 90% of children.
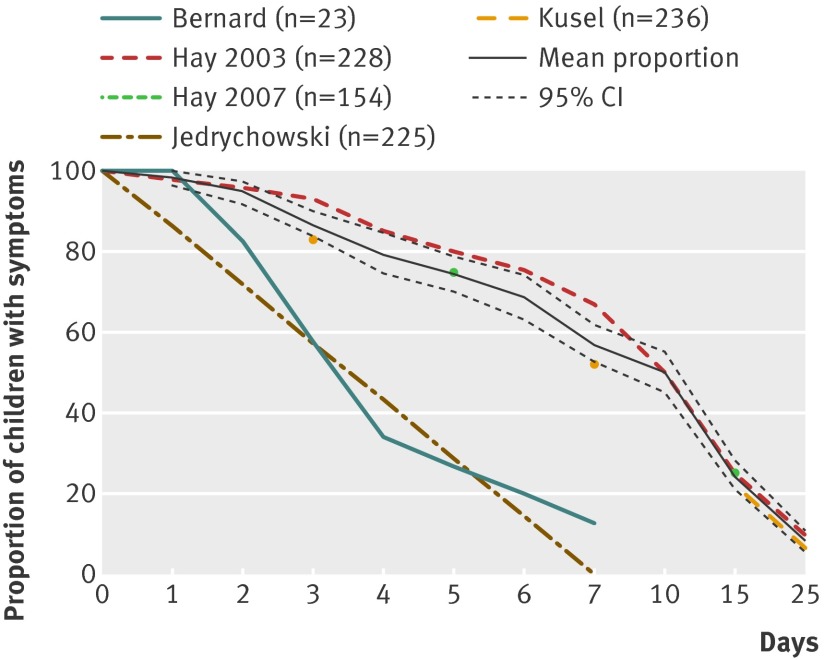
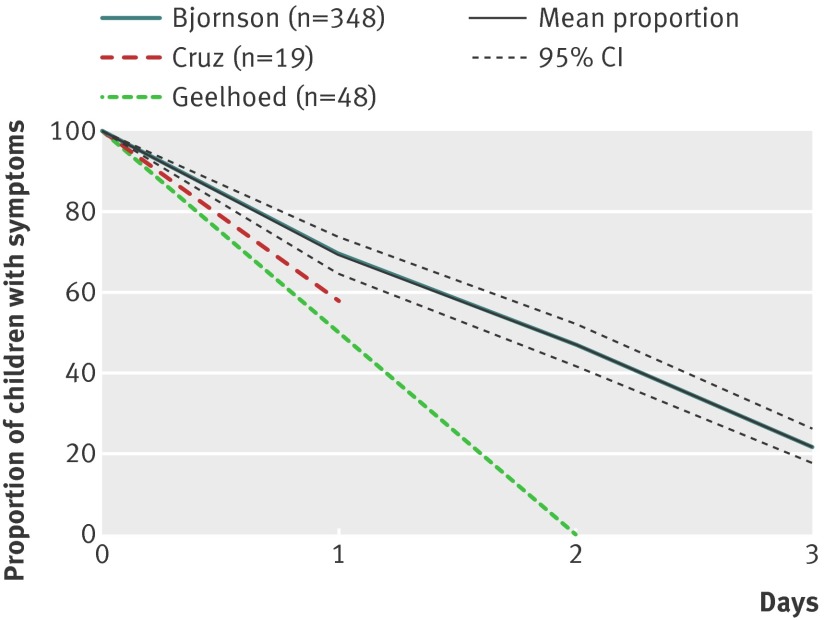
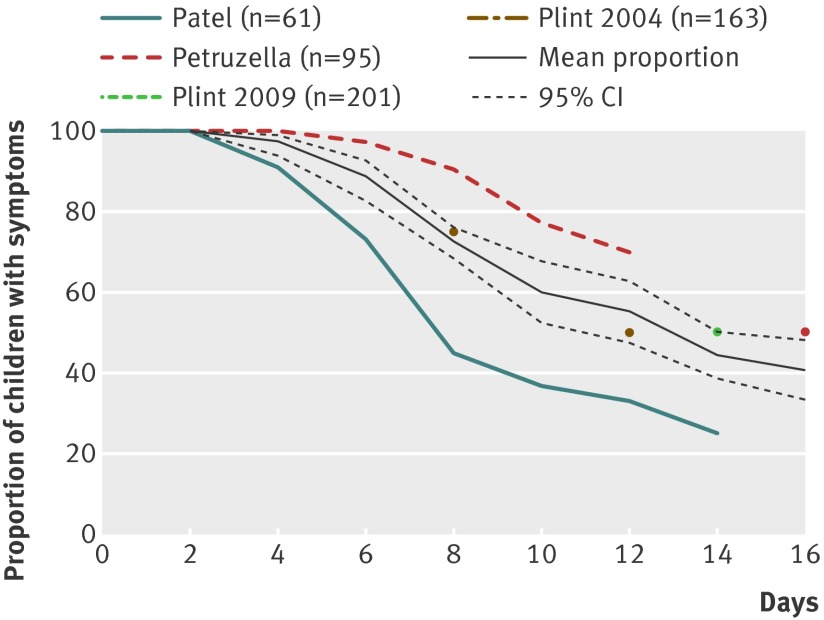
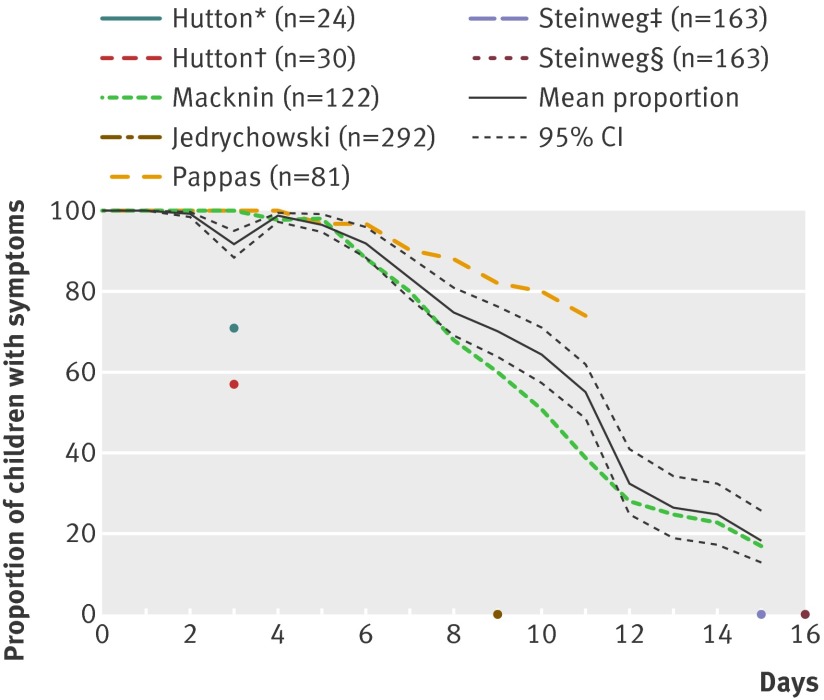
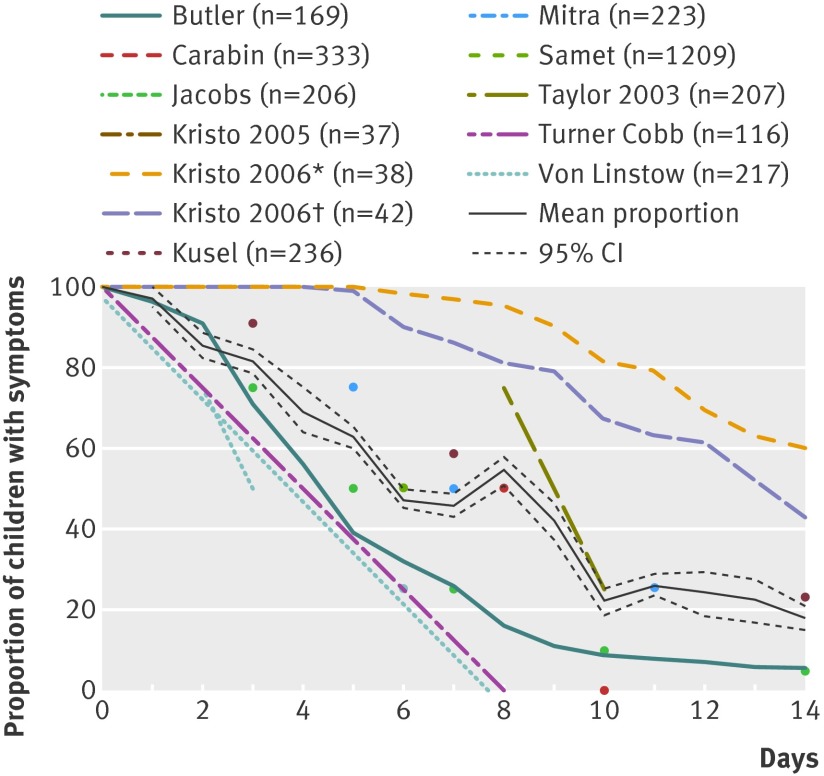
Results: Of 22,182 identified references, 23 trials and 25 observational studies met inclusion criteria. Study populations varied in age and duration of symptoms before study onset. In 90% of children, earache was resolved by seven to eight days, sore throat between two and seven days, croup by two days, bronchiolitis by 21 days, acute cough by 25 days, common cold by 15 days, and non-specific respiratory tract infections symptoms by 16 days.
Conclusions: The durations of earache and common colds are considerably longer than current guidance given to parents in the United Kingdom and the United States; for other symptoms such as sore throat, acute cough, bronchiolitis, and croup the current guidance is consistent with our findings. Updating current guidelines with new evidence will help support parents and clinicians in evidence based decision making for children with respiratory tract infections.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Prognosis of respiratory tract infections in primary care.BMJ. 2013 Dec 6;347:f7185. doi: 10.1136/bmj.f7185. BMJ. 2013. PMID: 24319258 No abstract available.
References
-
- Hay AD, Heron J, Ness A; ALSPAC study team. The prevalence of symptoms and consultations in pre-school children in the Avon Longitudinal Study of Parents and Children (ALSPAC): a prospective cohort study. Fam Pract 2005;22:367-74. - PubMed
-
- Fendrick A, Monto AS, Nightengale B, Sarnes M. The economic burden of non-influenza-related viral respiratory tract infection in the United States. Arch Intern Med 2003;163:487-94. - PubMed
-
- Hay AD, Wilson A, Fahey T, Peters TJ. The duration of acute cough in pre-school children presenting to primary care: a prospective cohort study. Fam Pract 2003;20:696-705. - PubMed
-
- Butler CC, Hood K, Kinnersley P, Robling M, Prout H, Houston H. Predicting the clinical course of suspected acute viral upper respiratory tract infection in children. Fam Pract 2005;22:92-5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous