

Red flags to screen for malignancy and fracture in patients with low back pain: systematic review
- PMID: 24335669
- PMCID: PMC3898572
- DOI: 10.1136/bmj.f7095
Red flags to screen for malignancy and fracture in patients with low back pain: systematic review
Erratum in
- BMJ. 2014;348:g7
Abstract
Objective: To review the evidence on diagnostic accuracy of red flag signs and symptoms to screen for fracture or malignancy in patients presenting with low back pain to primary, secondary, or tertiary care.
Design: Systematic review.
Data sources: Medline, OldMedline, Embase, and CINAHL from earliest available up to 1 October 2013.
Inclusion criteria: Primary diagnostic studies comparing red flags for fracture or malignancy to an acceptable reference standard, published in any language.
Review methods: Assessment of study quality and extraction of data was conducted by three independent assessors. Diagnostic accuracy statistics and post-test probabilities were generated for each red flag.
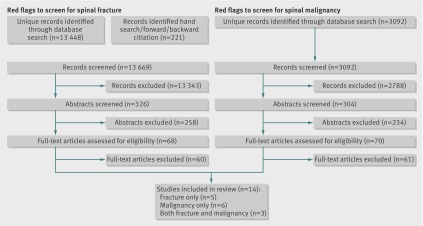
Results: We included 14 studies (eight from primary care, two from secondary care, four from tertiary care) evaluating 53 red flags; only five studies evaluated combinations of red flags. Pooling of data was not possible because of index test heterogeneity. Many red flags in current guidelines provide virtually no change in probability of fracture or malignancy or have untested diagnostic accuracy. The red flags with the highest post-test probability for detection of fracture were older age (9%, 95% confidence interval 3% to 25%), prolonged use of corticosteroid drugs (33%, 10% to 67%), severe trauma (11%, 8% to 16%), and presence of a contusion or abrasion (62%, 49% to 74%). Probability of spinal fracture was higher when multiple red flags were present (90%, 34% to 99%). The red flag with the highest post-test probability for detection of spinal malignancy was history of malignancy (33%, 22% to 46%).
Conclusions: While several red flags are endorsed in guidelines to screen for fracture or malignancy, only a small subset of these have evidence that they are indeed informative. These findings suggest a need for revision of many current guidelines.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures




Republished in
-
Red flags to screen for malignancy and fracture in patients with low back pain.Br J Sports Med. 2014 Oct;48(20):1518. doi: 10.1136/bjsports-2014-f7095rep. Br J Sports Med. 2014. PMID: 25257627
Comment in
-
Red flags for back pain.BMJ. 2013 Dec 12;347:f7432. doi: 10.1136/bmj.f7432. BMJ. 2013. PMID: 24336004 No abstract available.
-
["Red Flags" for back pain are not as threatening as the name suggests].Praxis (Bern 1994). 2014 Mar 26;103(7):411-2. doi: 10.1024/1661-8157/a001611. Praxis (Bern 1994). 2014. PMID: 24686764 German. No abstract available.
References
-
- Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2197-223. - PubMed
-
- Hoy D, Brooks P, Blyth F, Buchbinder R. The epidemiology of low back pain. Best Pract Res Clin Rheumatol 2010;24:769-81. - PubMed
-
- Williams CM, Henschke N, Maher CG, van Tulder MW, Koes BW, Macaskill P, et al. Red flags to screen for vertebral fracture in patients presenting with low-back pain. Cochrane Database Syst Rev 2013;1:CD008643. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical