

Progression-free survival as a surrogate endpoint for overall survival in glioblastoma: a literature-based meta-analysis from 91 trials
- PMID: 24335699
- PMCID: PMC3984546
- DOI: 10.1093/neuonc/not236
Progression-free survival as a surrogate endpoint for overall survival in glioblastoma: a literature-based meta-analysis from 91 trials
Abstract
Background: The aim of this study was to determine correlations between progression-free survival (PFS) and the objective response rate (ORR) with overall survival (OS) in glioblastoma and to evaluate their potential use as surrogates for OS.
Method: Published glioblastoma trials reporting OS and ORR and/or PFS with sufficient detail were included in correlative analyses using weighted linear regression.
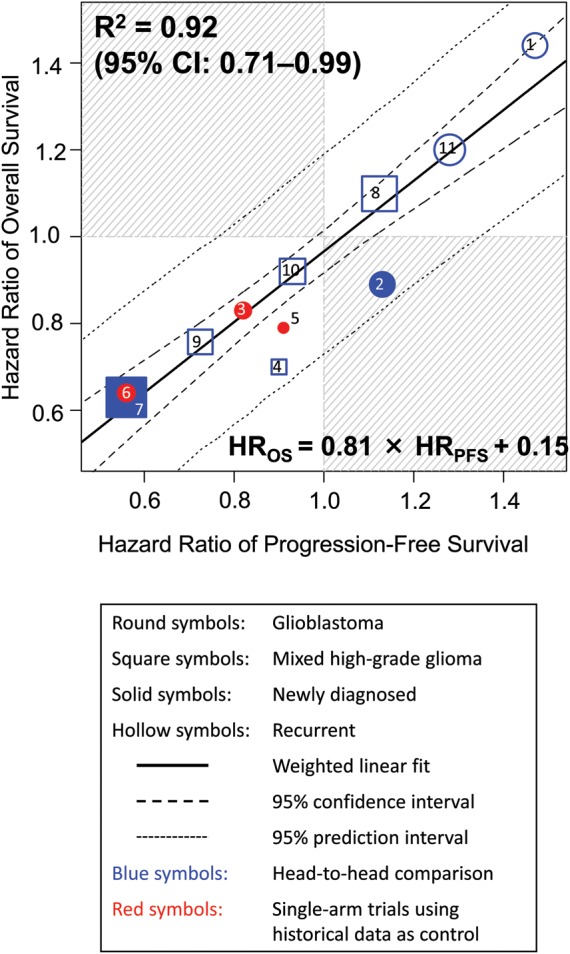
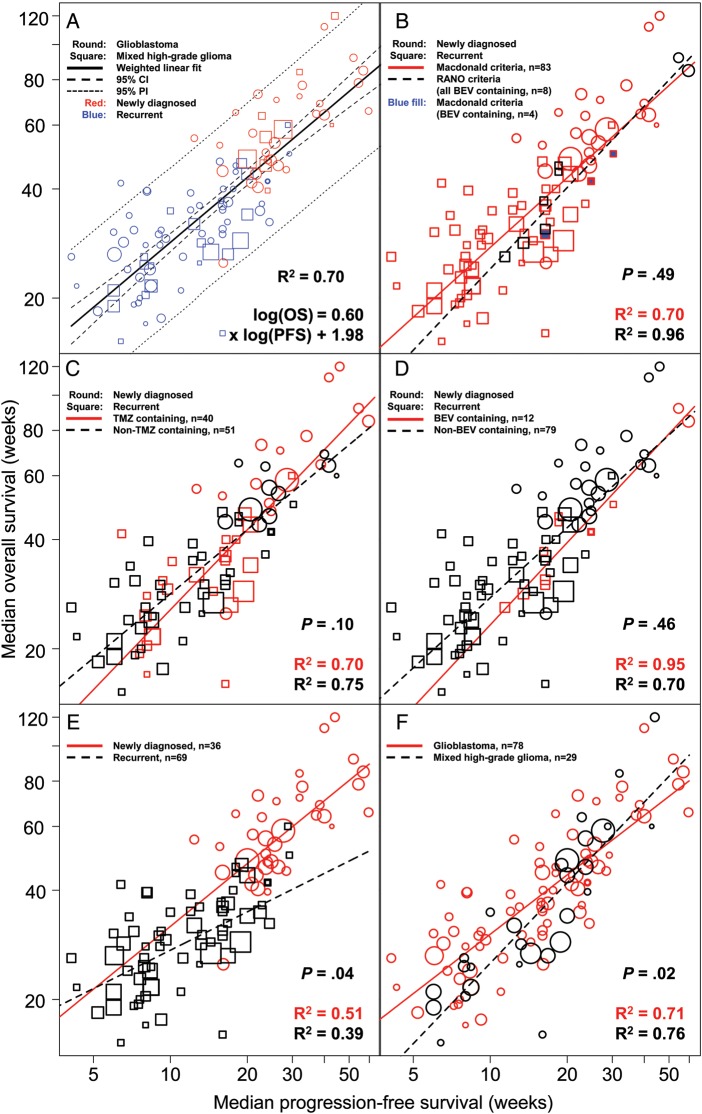
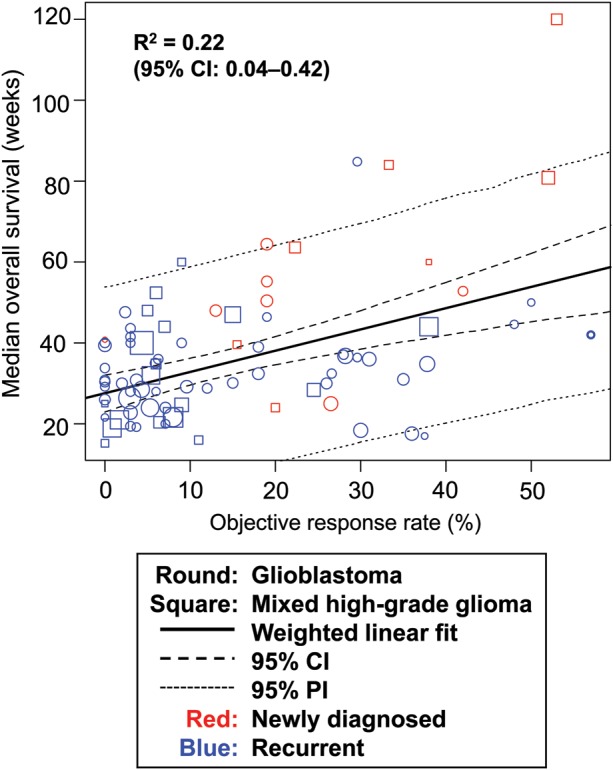
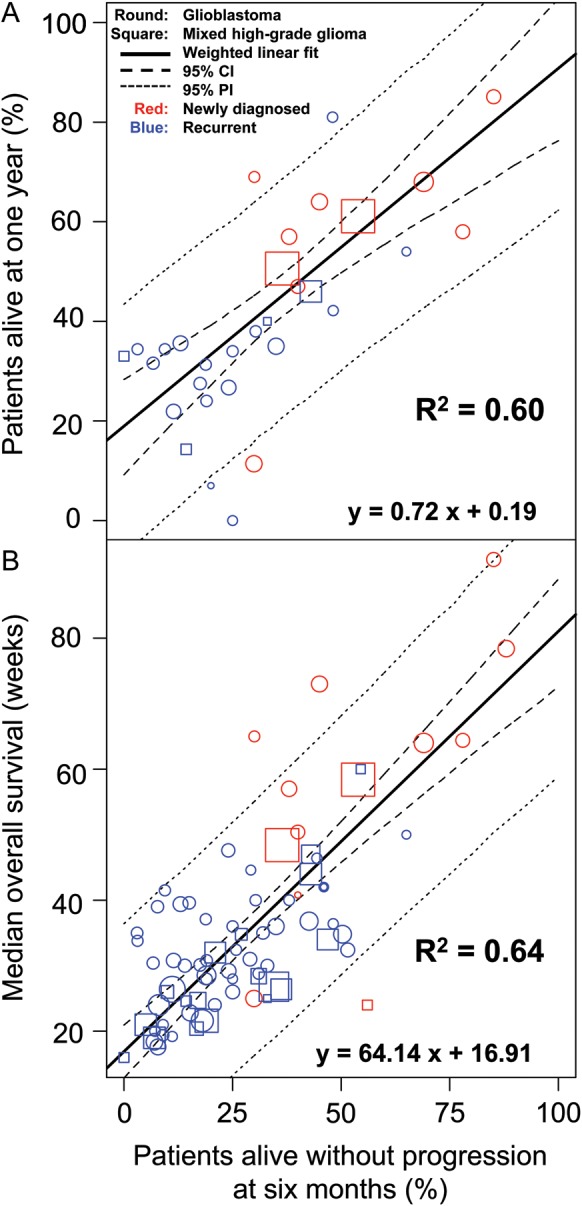
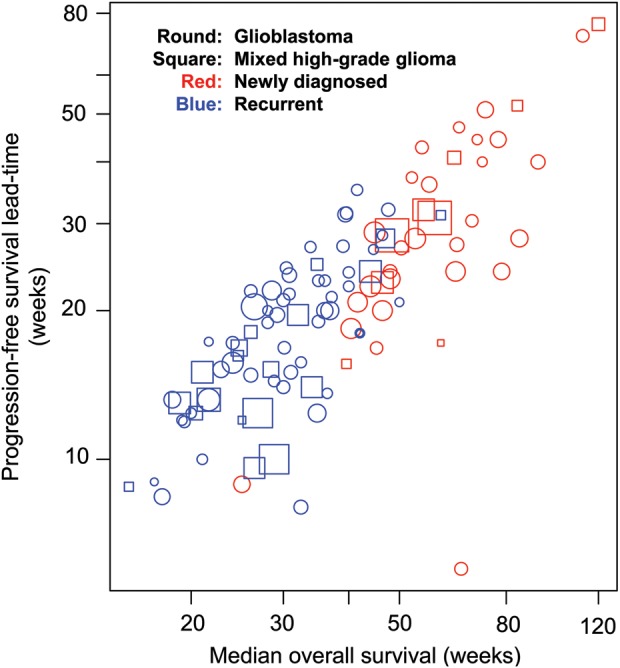
Results: Of 274 published unique glioblastoma trials, 91 were included. PFS and OS hazard ratios were strongly correlated; R(2) = 0.92 (95% confidence interval [CI], 0.71-0.99). Linear regression determined that a 10% PFS risk reduction would yield an 8.1% ± 0.8% OS risk reduction. R(2) between median PFS and median OS was 0.70 (95% CI, 0.59-0.79), with a higher value in trials using Response Assessment in Neuro-Oncology (RANO; R(2) = 0.96, n = 8) versus Macdonald criteria (R(2) = 0.70; n = 83). No significant differences were demonstrated between temozolomide- and bevacizumab-containing regimens (P = .10) or between trials using RANO and Macdonald criteria (P = .49). The regression line slope between median PFS and OS was significantly higher in newly diagnosed versus recurrent disease (0.58 vs 0.35, P = .04). R(2) for 6-month PFS with 1-year OS and median OS were 0.60 (95% CI, 0.37-0.77) and 0.64 (95% CI, 0.42-0.77), respectively. Objective response rate and OS were poorly correlated (R(2) = 0.22).
Conclusion: In glioblastoma, PFS and OS are strongly correlated, indicating that PFS may be an appropriate surrogate for OS. Compared with OS, PFS offers earlier assessment and higher statistical power at the time of analysis.
Keywords: glioblastoma; meta-analysis; overall survival; progression-free survival; regression; response rate; surrogate endpoint.
Figures
Comment in
-
Progression-free survival: too much risk, not enough reward?Neuro Oncol. 2014 May;16(5):615-6. doi: 10.1093/neuonc/nou041. Neuro Oncol. 2014. PMID: 24733851 Free PMC article. No abstract available.
References
-
- Tang PA, Bentzen SM, Chen EX, Siu LL. Surrogate end points for median overall survival in metastatic colorectal cancer: literature-based analysis from 39 randomized controlled trials of first-line chemotherapy. J Clin Oncol. 2007;25(29):4562–4568. - PubMed
-
- Saad ED, Katz A, Hoff PM, Buyse M. Progression-free survival as surrogate and as true end point: insights from the breast and colorectal cancer literature. Ann Oncol. 2010;21(1):7–12. - PubMed
-
- Johnson KR, Ringland C, Stokes BJ, et al. Response rate or time to progression as predictors of survival in trials of metastatic colorectal cancer or non-small-cell lung cancer: a meta-analysis. Lancet Oncol. 2006;7(9):741–746. - PubMed
-
- Hotta K, Fujiwara Y, Matsuo K, et al. Time to progression as a surrogate marker for overall survival in patients with advanced non-small cell lung cancer. J Thorac Oncol. 2009;4(3):311–317. - PubMed
-
- Buyse M, Burzykowski T, Carroll K, et al. Progression-free survival is a surrogate for survival in advanced colorectal cancer. J Clin Oncol. 2007;25(33):5218–5224. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
