

Heart failure and loss of metabolic control
- PMID: 24336014
- PMCID: PMC3980079
- DOI: 10.1097/FJC.0000000000000054
Heart failure and loss of metabolic control
Abstract
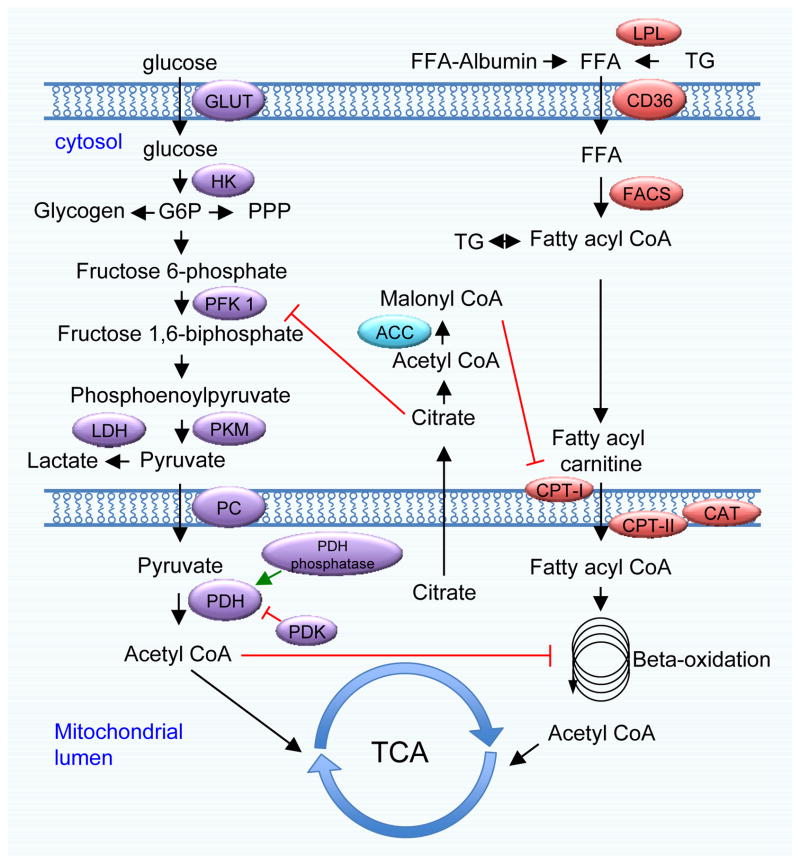
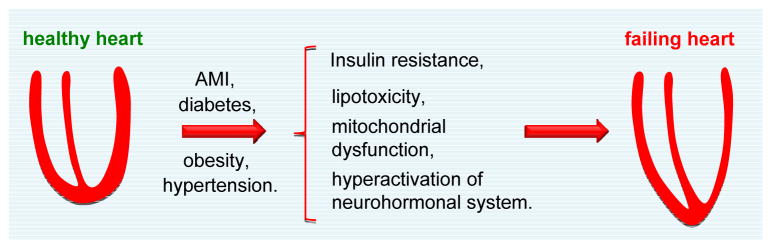
Heart failure is a leading cause of morbidity and mortality worldwide, currently affecting 5 million Americans. A syndrome defined on clinical terms, heart failure is the end result of events occurring in multiple heart diseases, including hypertension, myocardial infarction, genetic mutations and diabetes, and metabolic dysregulation, is a hallmark feature. Mounting evidence from clinical and preclinical studies suggests strongly that fatty acid uptake and oxidation are adversely affected, especially in end-stage heart failure. Moreover, metabolic flexibility, the heart's ability to move freely among diverse energy substrates, is impaired in heart failure. Indeed, impairment of the heart's ability to adapt to its metabolic milieu and associated metabolic derangement are important contributing factors in the heart failure pathogenesis. Elucidation of molecular mechanisms governing metabolic control in heart failure will provide critical insights into disease initiation and progression, raising the prospect of advances with clinical relevance.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB. Heart disease and stroke statistics--2013 update: A report from the american heart association. Circulation. 2013;127:e6–e245. - PMC - PubMed
-
- Stanley WC, Recchia FA, Lopaschuk GD. Myocardial substrate metabolism in the normal and failing heart. Physiol Rev. 2005;85:1093–1129. - PubMed
-
- Lopaschuk GD, Ussher JR, Folmes CD, Jaswal JS, Stanley WC. Myocardial fatty acid metabolism in health and disease. Physiol Rev. 2010;90:207–258. - PubMed
-
- Neubauer S. The failing heart--an engine out of fuel. N Engl J Med. 2007;356:1140–1151. - PubMed
-
- Tuunanen H, Knuuti J. Metabolic remodelling in human heart failure. Cardiovascular research. 2011;90:251–257. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
