

Dosing schedules for pneumococcal conjugate vaccine: considerations for policy makers
- PMID: 24336059
- PMCID: PMC3940379
- DOI: 10.1097/INF.0000000000000076
Dosing schedules for pneumococcal conjugate vaccine: considerations for policy makers
Abstract
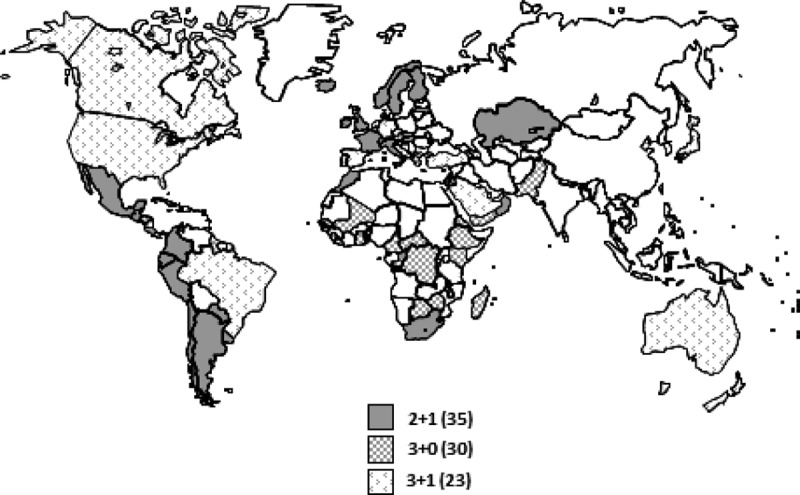
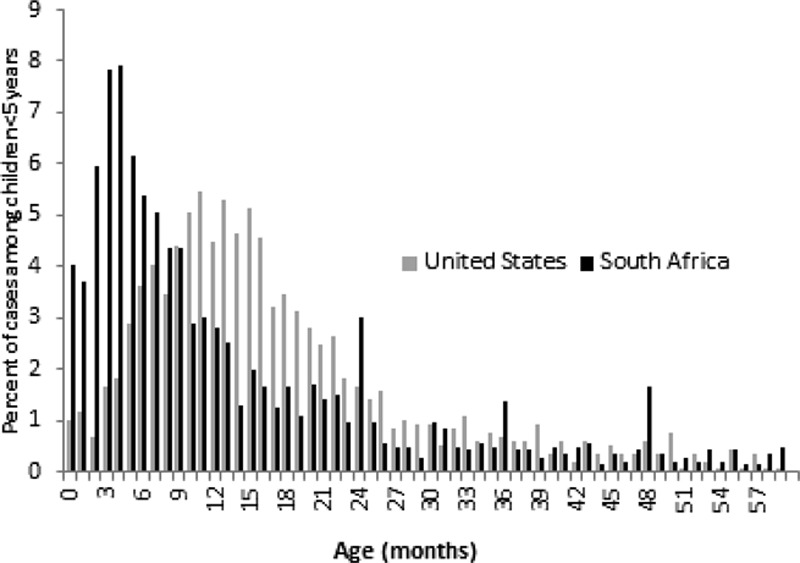
Since second generation pneumococcal conjugate vaccines (PCVs) targeting 10 and 13 serotypes became available in 2010, the number of national policy makers considering these vaccines has steadily increased. An important consideration for a national immunization program is the timing and number of doses-the schedule-that will best prevent disease in the population. Data on disease epidemiology and the efficacy or effectiveness of PCV schedules are typically considered when choosing a schedule. Practical concerns, such as the existing vaccine schedule, and vaccine program performance are also important. In low-income countries, pneumococcal disease and deaths typically peak well before the end of the first year of life, making a schedule that provides PCV doses early in life (eg, a 6-, 10- and 14-week schedule) potentially the best option. In other settings, a schedule including a booster dose may address disease that peaks in the second year of life or may be seen to enhance a schedule already in place. A large and growing body of evidence from immunogenicity studies, as well as clinical trials and observational studies of carriage, pneumonia and invasive disease, has been systematically reviewed; these data indicate that schedules of 3 or 4 doses all work well, and that the differences between these regimens are subtle, especially in a mature program in which coverage is high and indirect (herd) effects help enhance protection provided directly by a vaccine schedule. The recent World Health Organization policy statement on PCVs endorsed a schedule of 3 primary doses without a booster or, as a new alternative, 2 primary doses with a booster dose. While 1 schedule may be preferred in a particular setting based on local epidemiology or practical considerations, achieving high coverage with 3 doses is likely more important than the specific timing of doses.
Conflict of interest statement
Support for this project was provided by Program for Appropriate Technology in Health PATH) through funding from the GAVI. The views expressed by the authors do not necessarily reflect the views of the Centers for Disease Control and Prevention, GAVI and/or PATH. D.G.’s laboratory performs contract and or collaborative research for/with Pfizer, GlaxoSmithKline, Merck, Novartis and Sanofi Pasteur. D.G. has received travel or honorarium support for participation in external expert committees for Merck, Sanofi Pasteur, Pfizer and GlaxoSmithKline. K.O.B. received grant support from Pfizer and GlaxoSmithKline and has received travel or honorarium support for participation in external expert committees for Merck, Aventis-pasteur and GlaxoSmithKline. The authors have no other funding or conflicts of interest to declare.
Figures
References
-
- Centers for Disease Control and Prevention. Preventing pneumococcal disease among infants and young children: recommendations of the Advisory Committee on Immunization Practices (ACIP). Morb Mortal Wkly Rep. 2000;49(RR-9):1–35. - PubMed
-
- GAVI Alliance. GAVI Alliance. 2012. Available at: http://www.gavialliance.org/. Accessed December 6, 2012.
-
- World Health Organization, United Nations Childrens Fund. Global Action Plan for Prevention and Control of Pneumonia (GAPP) Geneva, Switzerland: WHO Press; 2009.
-
- Centers for Disease Control and Prevention. Prevention of pneumococcal disease among infants and children—use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine: recommendations of the Advisory Committee on Immunization Practices (ACIP). Morb Mortal Wkly Rep. 2010;59(RR11):1–18. - PubMed
-
- Black S, Shinefield H, Fireman B, et al. Efficacy, safety and immunogenicity of heptavalent pneumococcal conjugate vaccine in children. Northern California Kaiser Permanente Vaccine Study Center Group. Pediatr Infect Dis J. 2000;19:187–195. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
