

Haploinsufficiency of CSF-1R and clinicopathologic characterization in patients with HDLS
- PMID: 24336230
- PMCID: PMC3937843
- DOI: 10.1212/WNL.0000000000000046
Haploinsufficiency of CSF-1R and clinicopathologic characterization in patients with HDLS
Abstract
Objective: To clarify the genetic, clinicopathologic, and neuroimaging characteristics of patients with hereditary diffuse leukoencephalopathy with spheroids (HDLS) with the colony stimulating factor 1 receptor (CSF-1R) mutation.
Methods: We performed molecular genetic analysis of CSF-1R in patients with HDLS. Detailed clinical and neuroimaging findings were retrospectively investigated. Five patients were examined neuropathologically.
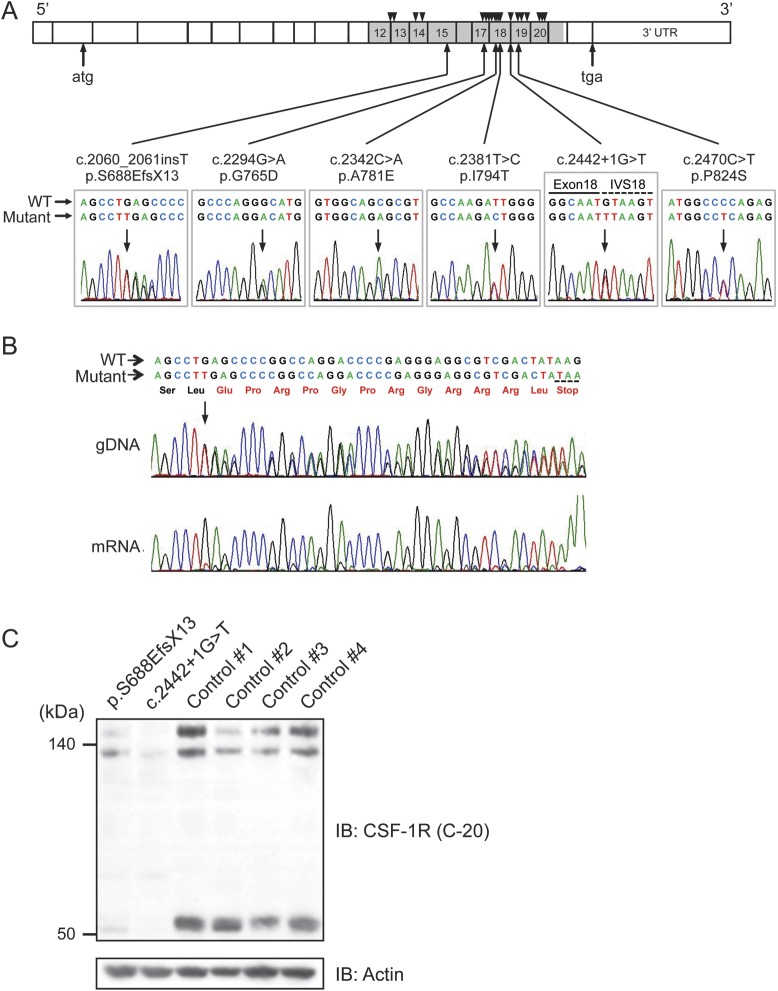
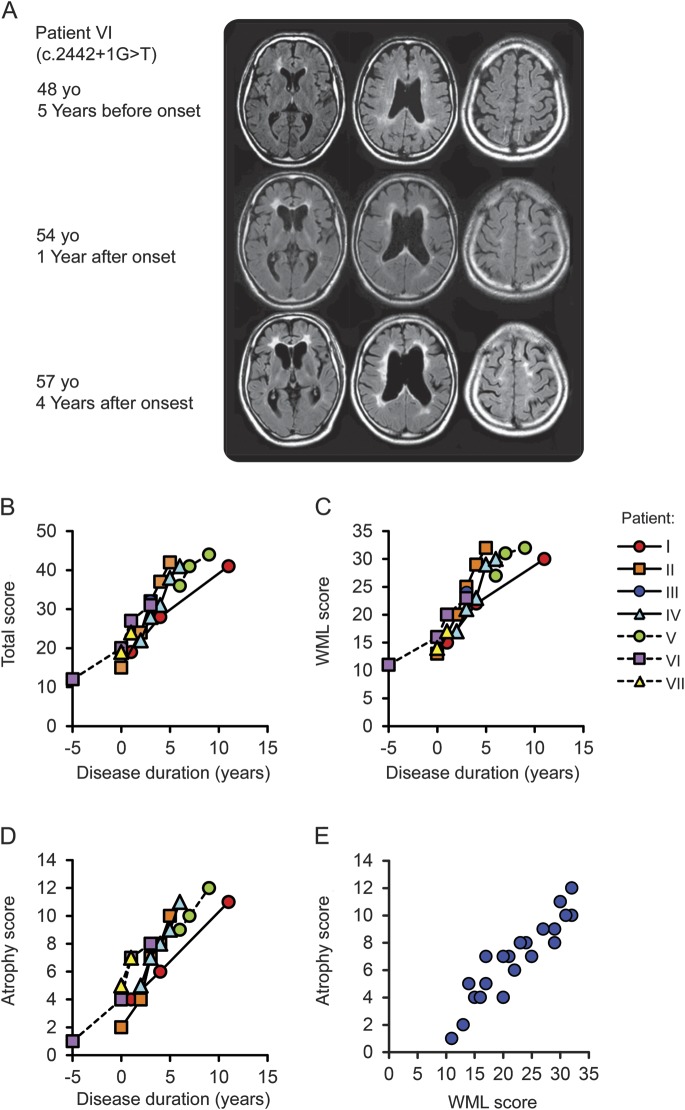
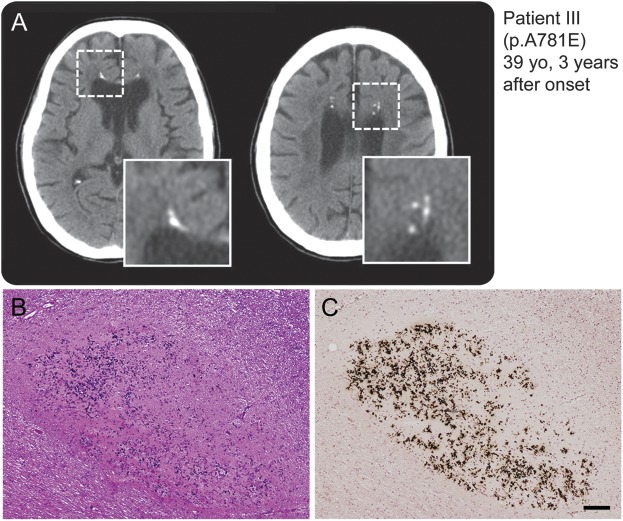
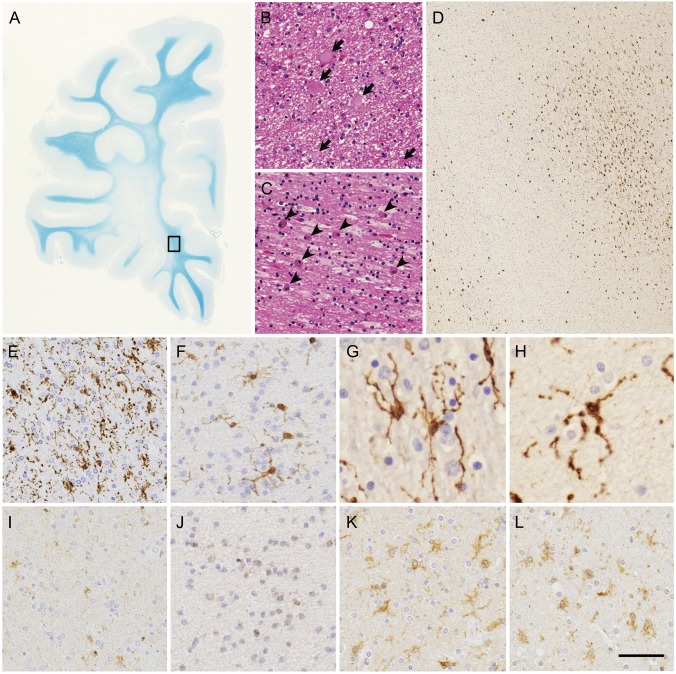
Results: We found 6 different CSF-1R mutations in 7 index patients from unrelated Japanese families. The CSF-1R mutations included 3 novel mutations and 1 known missense mutation at evolutionarily conserved amino acids, and 1 novel splice-site mutation. We identified a novel frameshift mutation. Reverse transcription PCR analysis revealed that the frameshift mutation causes nonsense-mediated mRNA decay by generating a premature stop codon, suggesting that haploinsufficiency of CSF-1R is sufficient to cause HDLS. Western blot analysis revealed that the expression level of CSF-1R in the brain from the patients was lower than from control subjects. The characteristic MRI findings were the involvement of the white matter and thinning of the corpus callosum with signal alteration, and sequential analysis revealed that the white matter lesions and cerebral atrophy relentlessly progressed with disease duration. Spotty calcifications in the white matter were frequently observed by CT. Neuropathologic analysis revealed that microglia in the brains of the patients demonstrated distinct morphology and distribution.
Conclusions: These findings suggest that patients with HDLS, irrespective of mutation type in CSF-1R, show characteristic clinical and neuroimaging features, and that perturbation of CSF-1R signaling by haploinsufficiency may play a role in microglial dysfunction leading to the pathogenesis of HDLS.
Figures
Comment in
-
Hereditary diffuse leukoencephalopathy with axonal spheroids: more than just a rare disease.Neurology. 2014 Jan 14;82(2):102-3. doi: 10.1212/WNL.0000000000000026. Epub 2013 Dec 13. Neurology. 2014. PMID: 24336229 No abstract available.
References
-
- Axelsson R, Röyttä M, Sourander P, Akesson HO, Andersen O. Hereditary diffuse leukoencephalopathy with spheroids. Acta Psychiatr Scand Suppl 1984;314:1–65 - PubMed
-
- Wong JC, Chow TW, Hazrati LN. Adult-onset leukoencephalopathy with axonal spheroids and pigmented glia can present as frontotemporal dementia syndrome. Dement Geriatr Cogn Disord 2011;32:150–158 - PubMed
-
- Kinoshita M, Yoshida K, Oyanagi K, Hashimoto T, Ikeda S. Hereditary diffuse leukoencephalopathy with axonal spheroids caused by R782H mutation in CSF1R: case report. J Neurol Sci 2012;318:115–118 - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous