

Sex differences in the incidence of chronic myeloid leukemia
- PMID: 24337217
- PMCID: PMC3943788
- DOI: 10.1007/s00411-013-0507-4
Sex differences in the incidence of chronic myeloid leukemia
Abstract
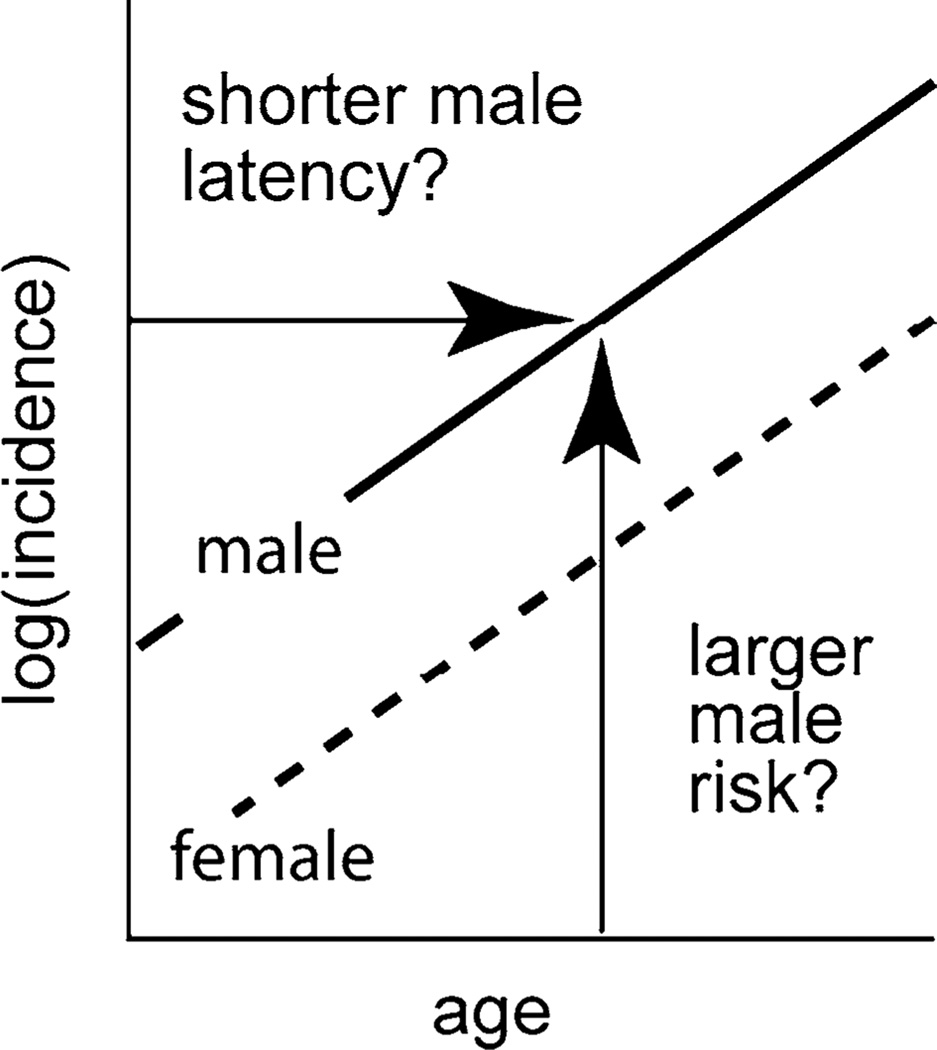
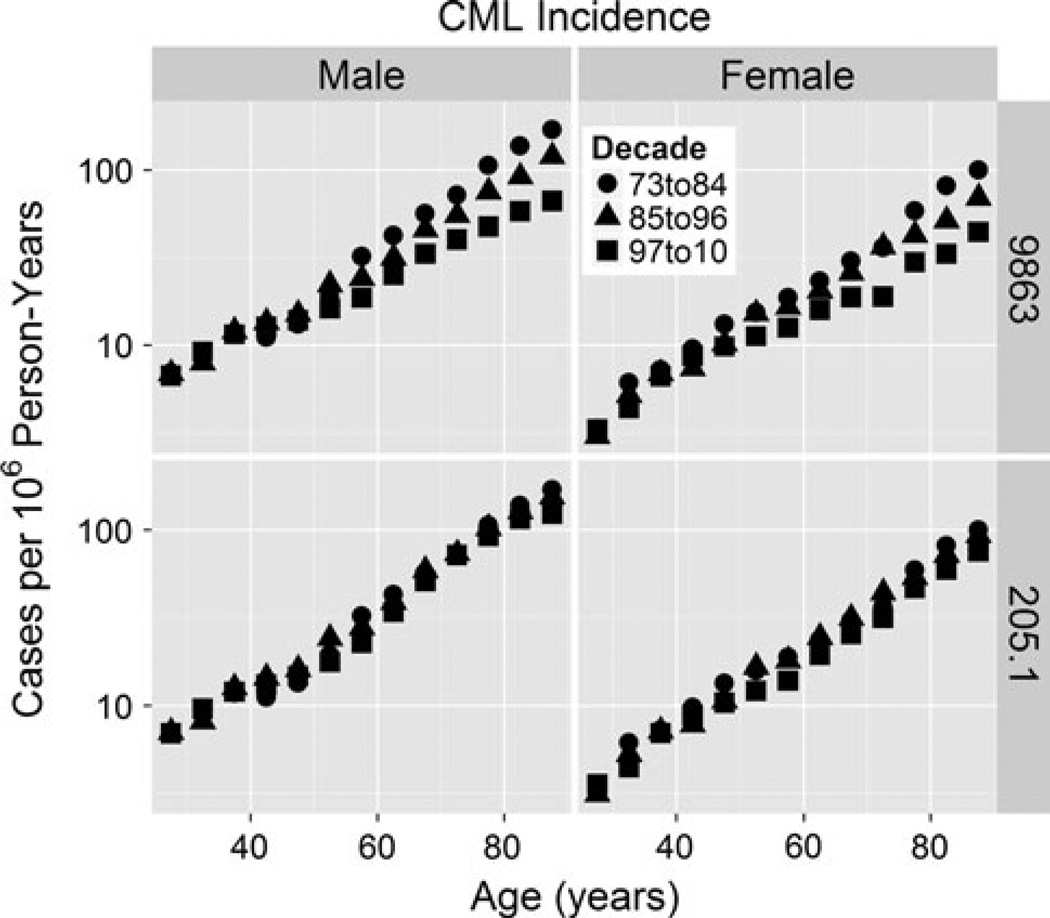
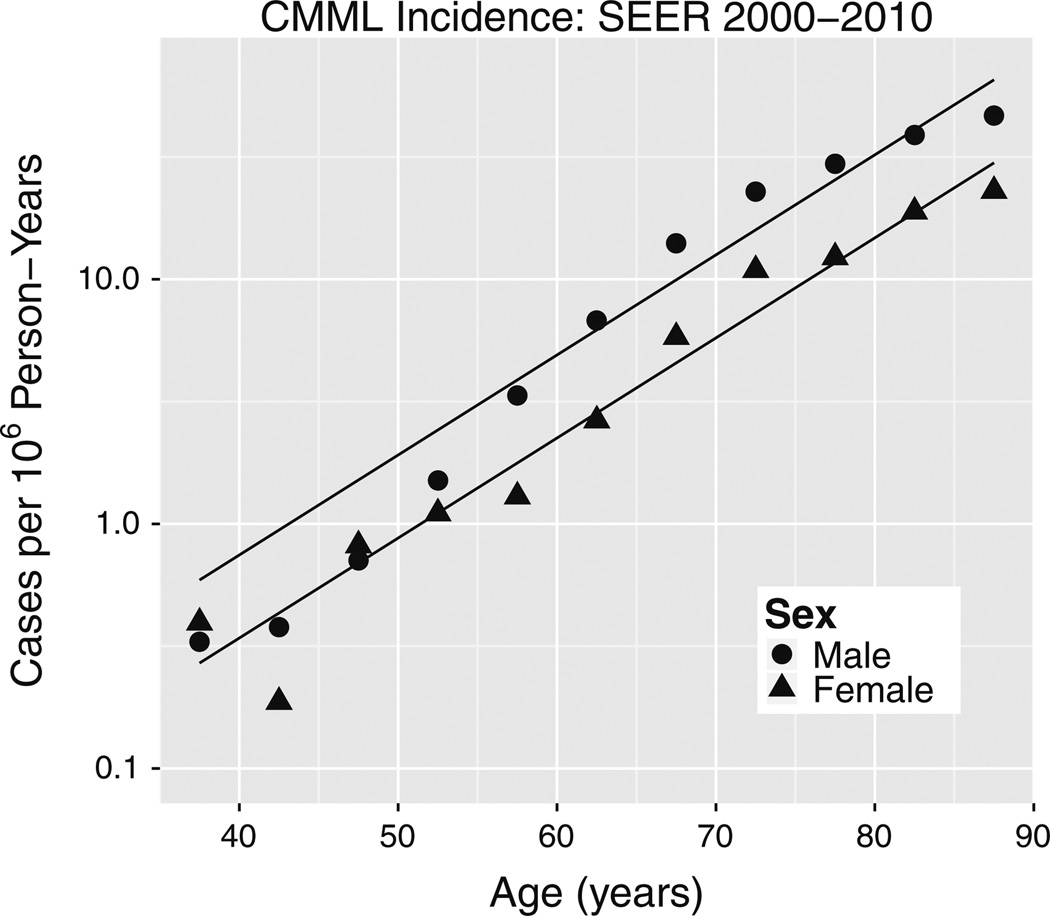
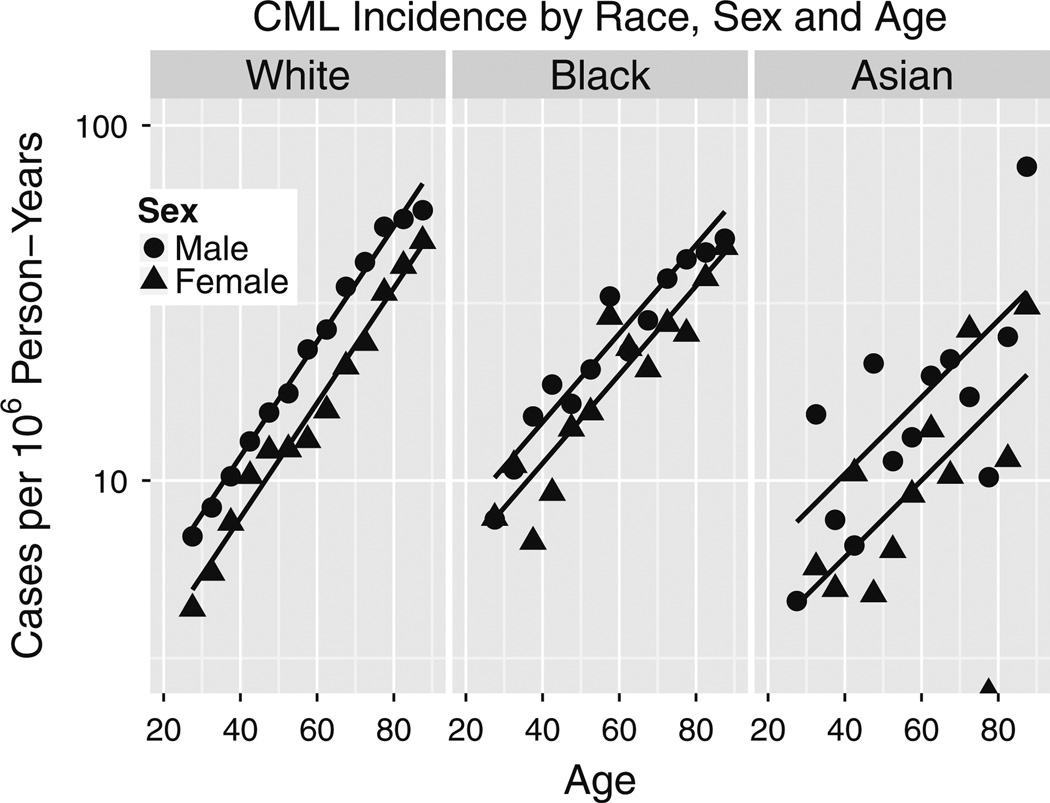
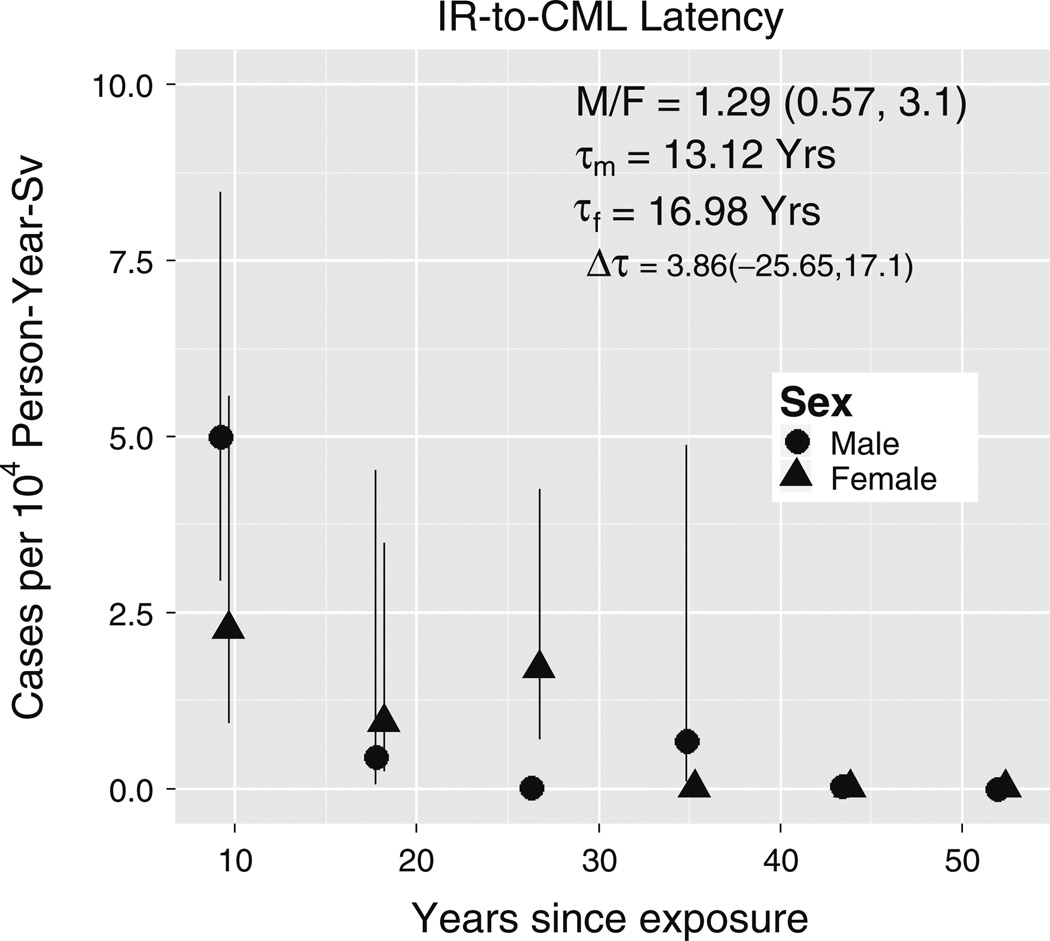
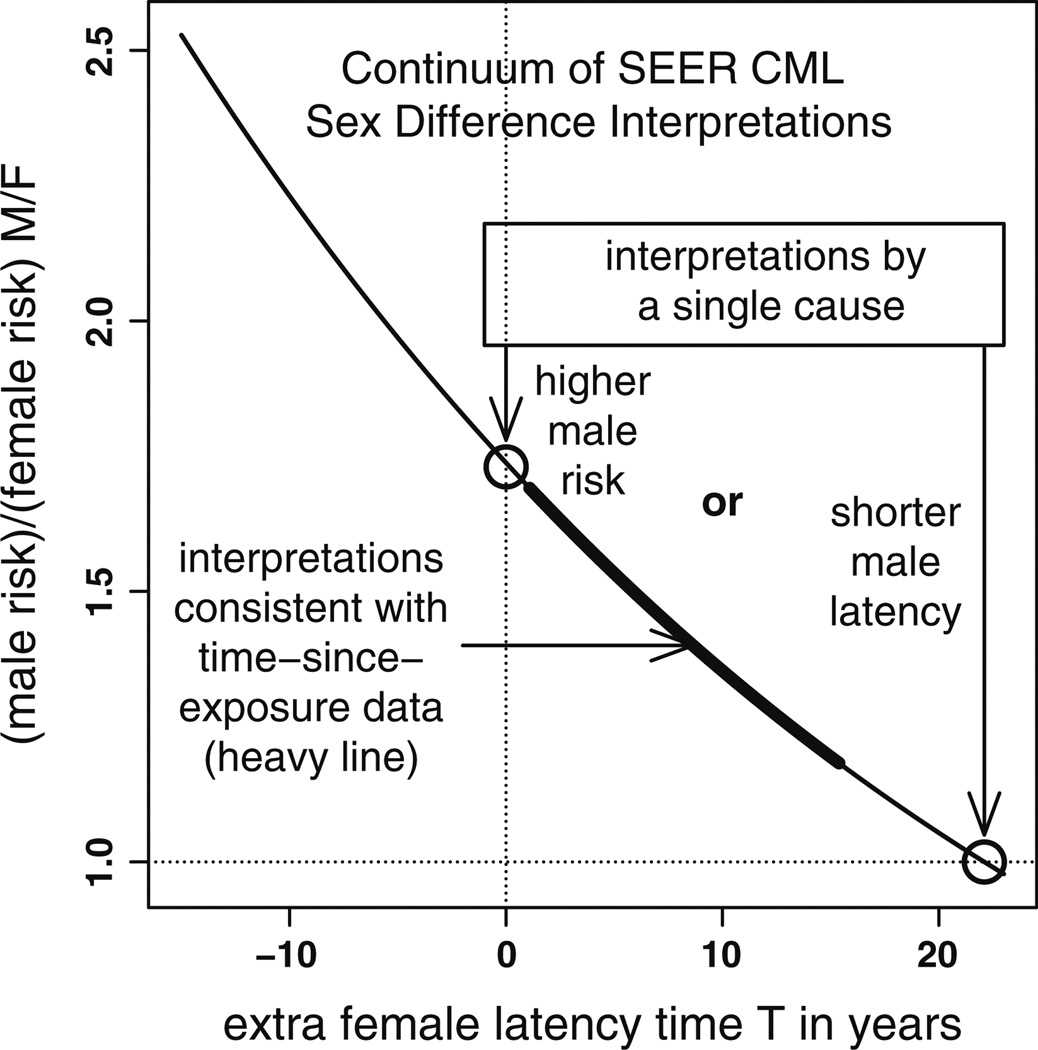
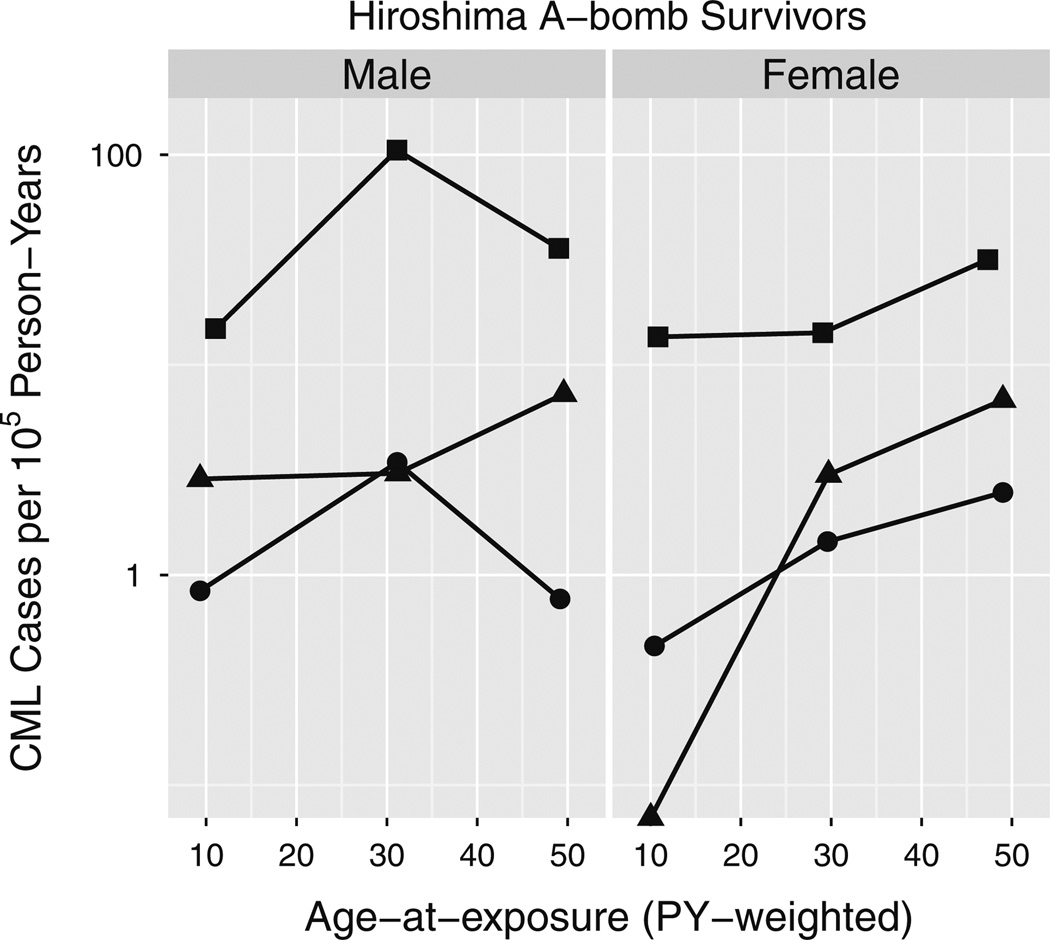
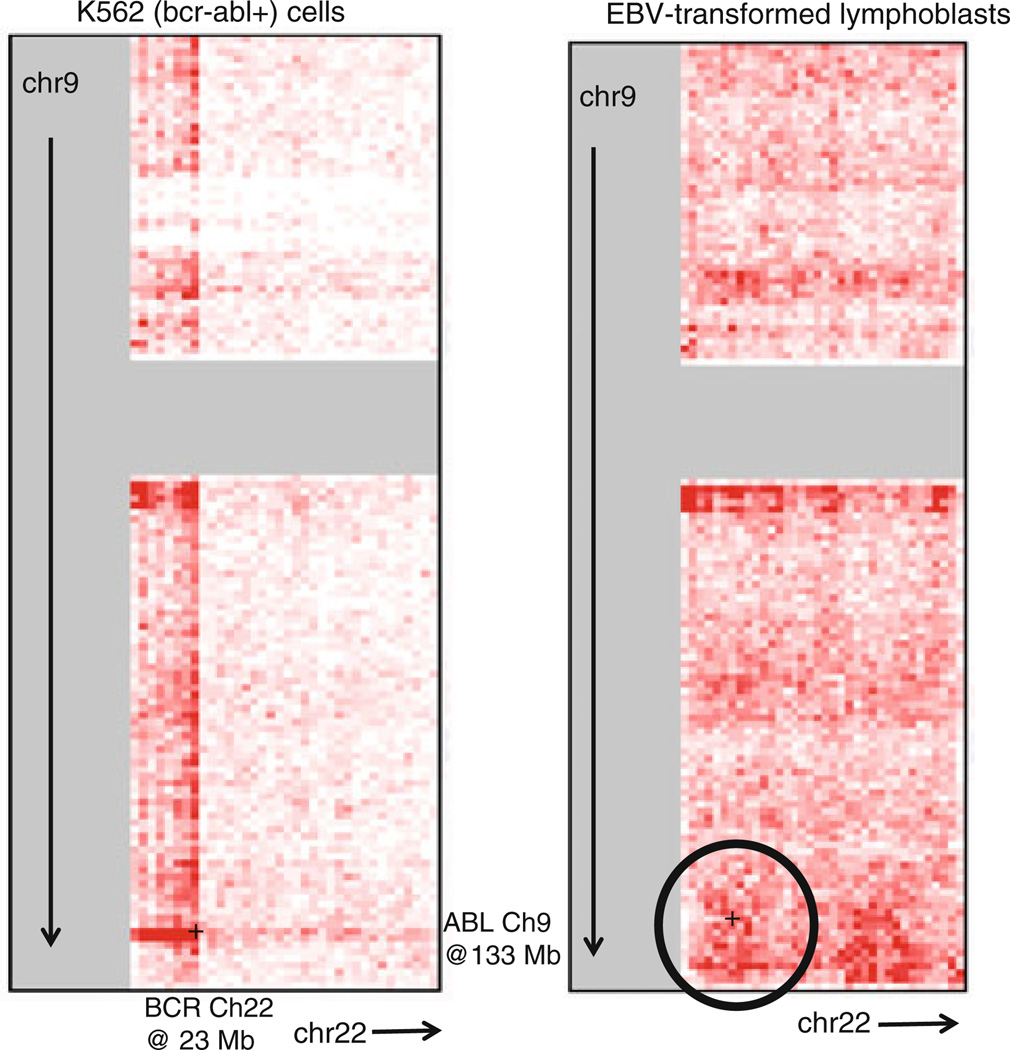
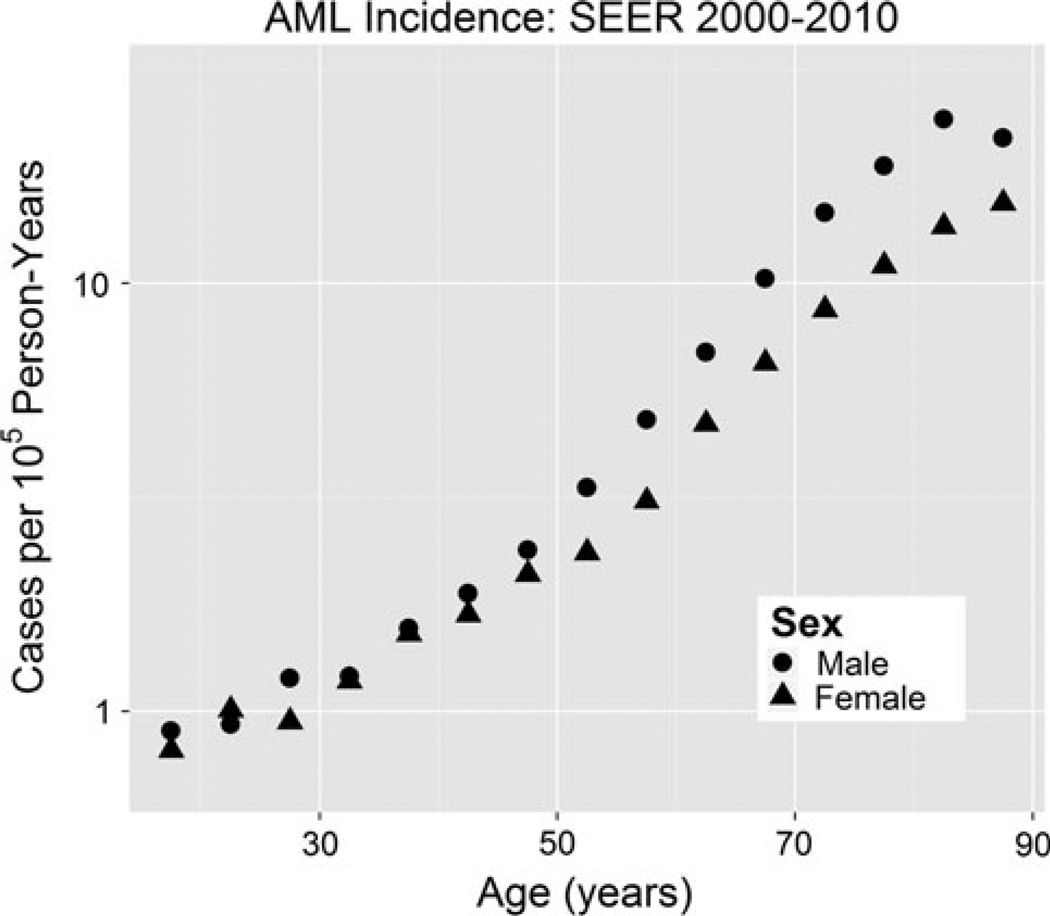
The incidence of chronic myeloid leukemia (CML), which is caused by BCR/ABL chimeric oncogene formation in a pluripotent hematopoietic stem cell (HSC), increases with age and exposure to ionizing radiation. CML is a comparatively well-characterized neoplasm, important for its own sake and useful for insights into other neoplasms. Here, Surveillance, Epidemiology and End Results (SEER) CML data are analyzed after considering possible misclassification of chronic myelo-monocytic leukemia as CML. For people older than 25 years, plots of male and female CML log incidences versus age at diagnosis are approximately parallel straight lines with males either above or to the left of females. This is consistent with males having a higher risk of developing CML or a shorter latency from initiation to diagnosis of CML. These distinct mechanisms cannot be distinguished using SEER data alone. Therefore, CML risks among male and female Japanese A-bomb survivors are also analyzed. The present analyses suggest that sex differences in CML incidence more likely result from differences in risk than in latency. The simplest but not the sole interpretation of this is that males have more target cells at risk to develop CML. Comprehensive mathematical models of CML could lead to a better understanding of the role of HSCs in CML and other preleukemias that can progress to acute leukemia.
Conflict of interest statement
Figures

References
-
- Akaike H. A new look at the statistical model identification. IEEE Trans Autom Control. 1974;19:716–723.
-
- Beheshti A, Sachs RK, Peluso M, Rietman E, Hahnfeldt P, Hlatky L. Age and space irradiation modulate tumor progression: implications for carcinogenesis risk. Radiat Res. 2013;179(2):208–220. - PubMed
-
- Bjorkholm M, Ohm L, Eloranta S, Derolf A, Hultcrantz M, Sjoberg J, Andersson T, Hoglund M, Richter J, Landgren O, Kristinsson SY, Dickman PW. Success story of targeted therapy in chronic myeloid leukemia: a population-based study of patients diagnosed in Sweden from 1973 to 2008. J Clin Oncol. 2011;29(18):2514–2520. - PMC - PubMed
-
- Braun WJ, Murdoch DJ. A first course in statistical programming with R. Cambridge: Cambridge University Press; 2007.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
