

Dietary therapy mitigates persistent wake deficits caused by mild traumatic brain injury
- PMID: 24337480
- PMCID: PMC3951738
- DOI: 10.1126/scitranslmed.3007092
Dietary therapy mitigates persistent wake deficits caused by mild traumatic brain injury
Abstract
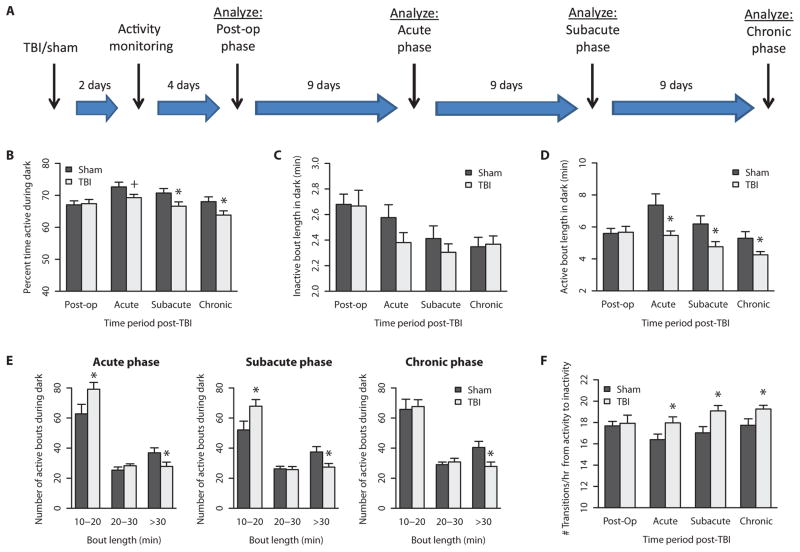
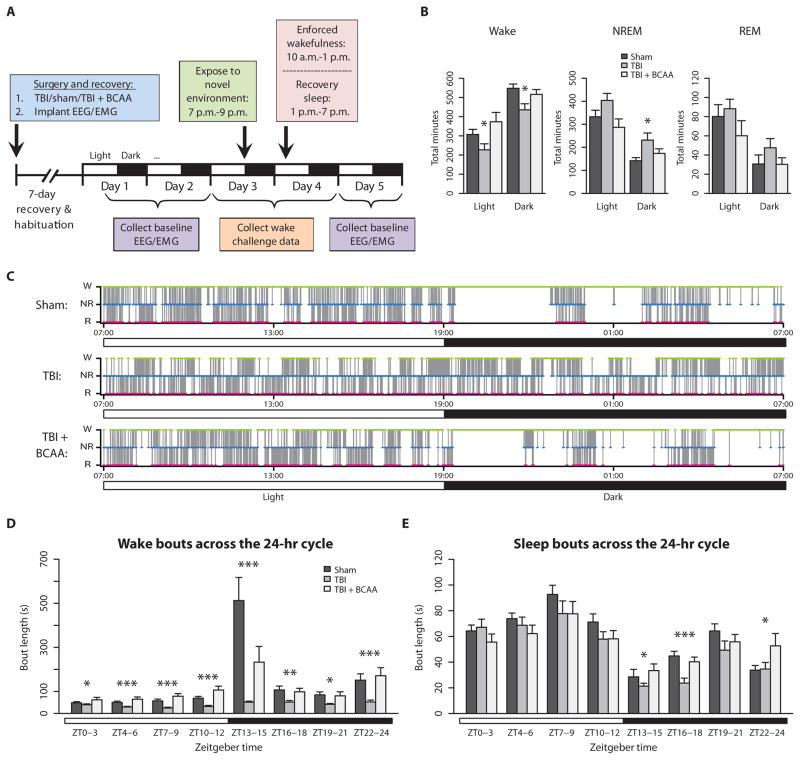
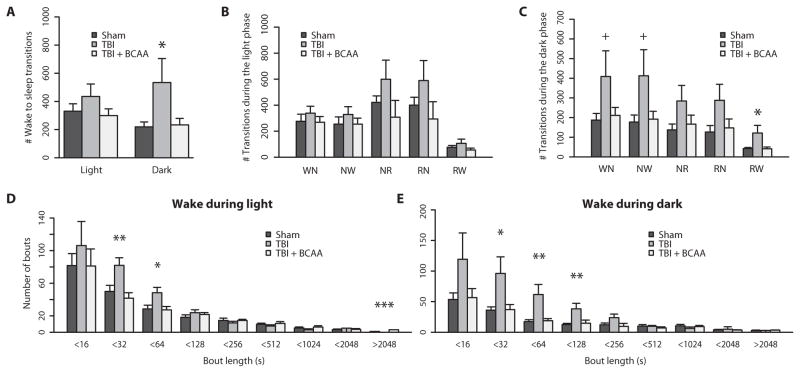
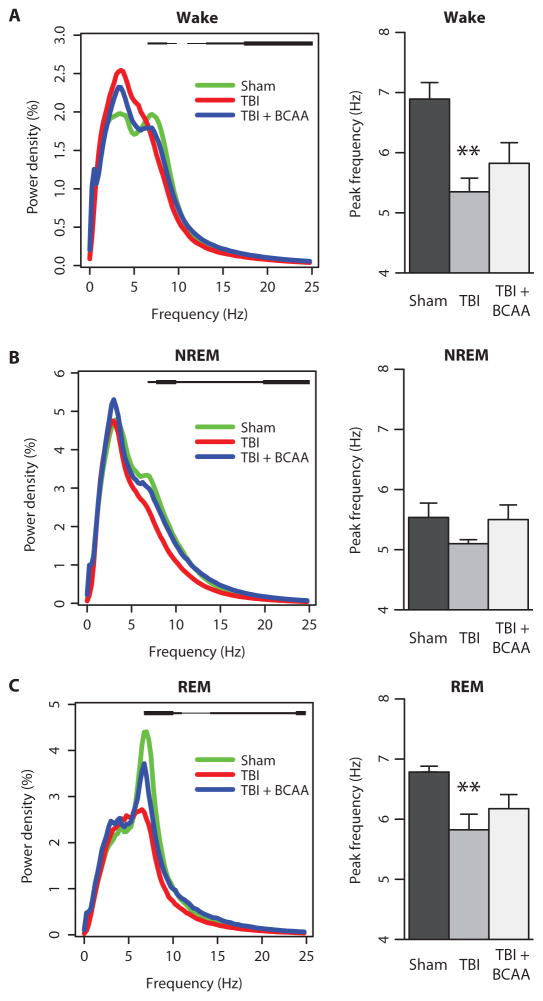
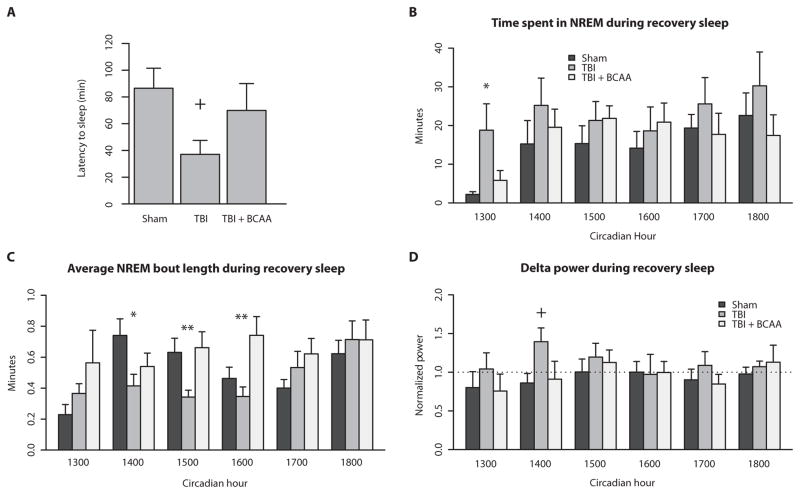
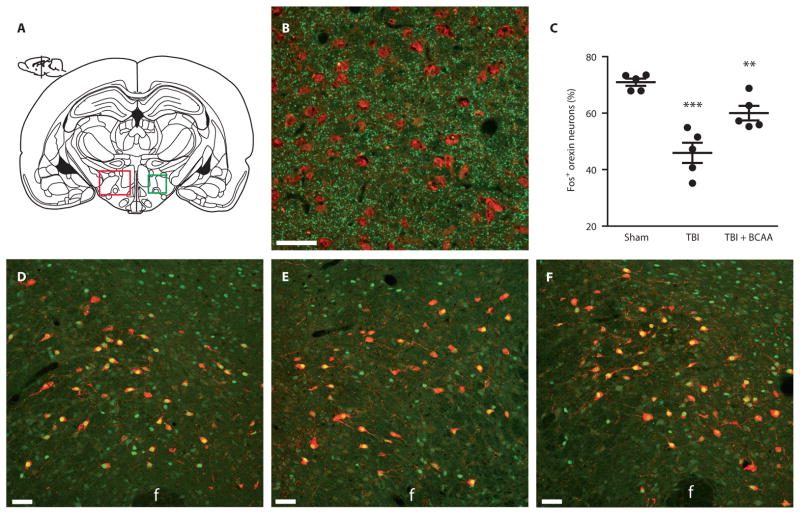
Sleep disorders are highly prevalent in patients with traumatic brain injury (TBI) and can significantly impair cognitive rehabilitation. No proven therapies exist to mitigate the neurocognitive consequences of TBI. We show that mild brain injury in mice causes a persistent inability to maintain wakefulness and decreases orexin neuron activation during wakefulness. We gave mice a dietary supplement of branched-chain amino acids (BCAAs), precursors for de novo glutamate synthesis in the brain. BCAA therapy reinstated activation of orexin neurons and improved wake deficits in mice with mild brain injury. Our data suggest that dietary BCAA intervention, acting in part through orexin, can ameliorate injury-induced sleep disturbances and may facilitate cognitive rehabilitation after brain injury.
Conflict of interest statement
Figures
References
-
- Castriotta RJ, Murthy JN. Sleep disorders in patients with traumatic brain injury: A review. CNS Drugs. 2011;25:175–185. - PubMed
-
- Baumann CR, Werth E, Stocker R, Ludwig S, Bassetti CL. Sleep-wake disturbances 6 months after traumatic brain injury: A prospective study. Brain. 2007;130:1873–1883. - PubMed
-
- Kempf J, Werth E, Kaiser PR, Bassetti CL, Baumann CR. Sleep-wake disturbances 3 years after traumatic brain injury. J Neurol Neurosurg Psychiatry. 2010;81:1402–1405. - PubMed
-
- Makley MJ, English JB, Drubach DA, Kreuz AJ, Celnik PA, Tarwater PM. Prevalence of sleep disturbance in closed head injury patients in a rehabilitation unit. Neurorehabil Neural Repair. 2008;22:341–347. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
