

Defining incidence and risk factors of venous thromboemolism after hepatectomy
- PMID: 24337986
- PMCID: PMC4031260
- DOI: 10.1007/s11605-013-2432-x
Defining incidence and risk factors of venous thromboemolism after hepatectomy
Erratum in
- J Gastrointest Surg. 2014 Apr;18(4):887. Kheng, Marian [corrected to Kheng, Marin]
Abstract
Background: The incidence of venous thromboembolism (VTE) among patients undergoing hepatic surgery is poorly defined, leading to varied use of VTE prophylaxis among surgeons. We sought to define the incidence of VTE after liver surgery and identify risk factors associated with VTE.
Methods: Incidence of VTE and associated risk factors within 90 days of hepatic resection between 2006 and 2012 at a major academic center was analyzed. Risk factors for VTE were identified using univariate and multivariate analyses.
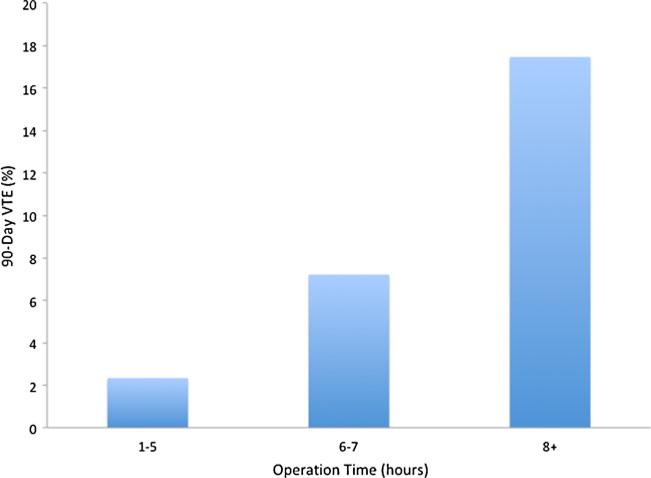
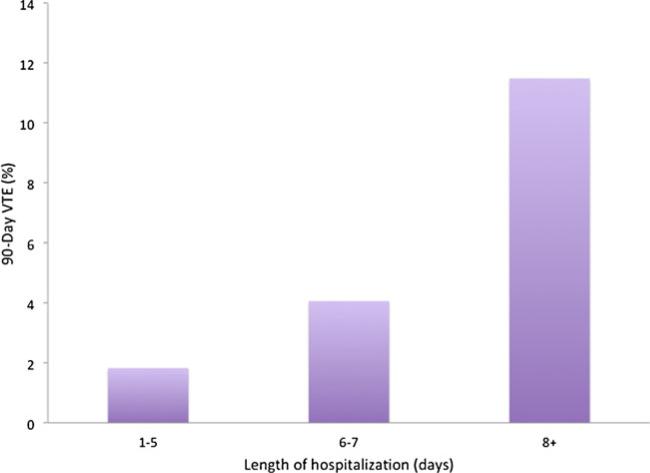
Results: A total of 599 patients were included in the study cohort; 30 (5.0 %) had a prior history of VTE. The indications for surgery were malignant (90.8 %) and benign lesions (9.2 %). The majority of patients underwent a minor hepatectomy (<3 Couinaud segments; n = 402, 67.1 %) while 195 (32.6 %) patients underwent a major hepatectomy (≥3 Couinaud segments). Three hundred seven (51.3 %) patients were started on VTE chemoprophylaxis preoperatively with 407 (67.8 %) patients receiving VTE chemoprophylaxis within 24 h of surgery. Twenty-eight (4.7 %) patients developed VTE; 20 (3.3 %) had deep venous thrombosis (DVT), 11 (1.8 %) had pulmonary embolism (PE), and three (0.5 %) developed both DVT and PE. Among the VTE patients, 23 (82.1 %) had received VTE chemoprophylaxis. On multivariate analyses, history of VTE (odds ratio [OR] 4.51, 95 % confidence interval [CI] 1.81-17.22, P = 0.03), prolonged operative time (OR 1.17 per additional hour, 95 % CI 1.04-1.32, P = 0.009), and increased length of stay (LOS) (OR 1.07, 95 % CI 1.02-1.12, P = 0.01) were independent risk factors for VTE.
Conclusion: VTE within 90 days of hepatic resection is common, occurring in nearly one in 20 patients. Most VTE events occurred among patients who received current best practice prophylaxis for VTE. More aggressive strategies to identify and reduce the risk of VTE in patients at highest risk of VTE, including those with a history of VTE, extended operative time, and prolonged LOS, are warranted.
Figures

References
-
- Collins R, Scrimgeour A, Yusuf S, Peto R. Reduction in fatal pulmonary embolism and venous thrombosis by perioperative administration of subcutaneous heparin. Overview of results of randomized trials in general, orthopedic, and urologic surgery. N Engl J Med. 1988;318(18):1162–73. - PubMed
-
- Mismetti P, Laporte S, Darmon JY, et al. Meta-analysis of low molecular weight heparin in the prevention of venous thromboembolism in general surgery. Br J Surg. 2001;88(7):913–30. - PubMed
-
- Caprini JA, Arcelus JI, Hasty JH, et al. Clinical assessment of venous thromboembolic risk in surgical patients. Semin Thromb Hemost. 1991;17(Suppl 3):304–12. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
