

Techniques and outcomes of minimally invasive trabecular ablation and bypass surgery
- PMID: 24338085
- PMCID: PMC4108346
- DOI: 10.1136/bjophthalmol-2013-304256
Techniques and outcomes of minimally invasive trabecular ablation and bypass surgery
Abstract
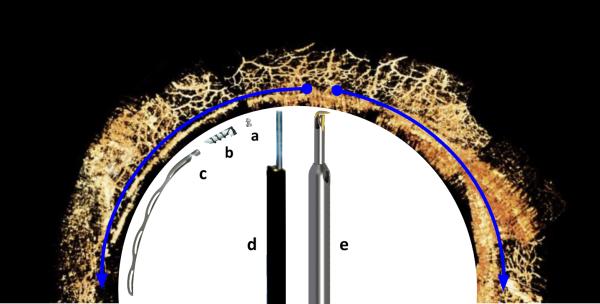
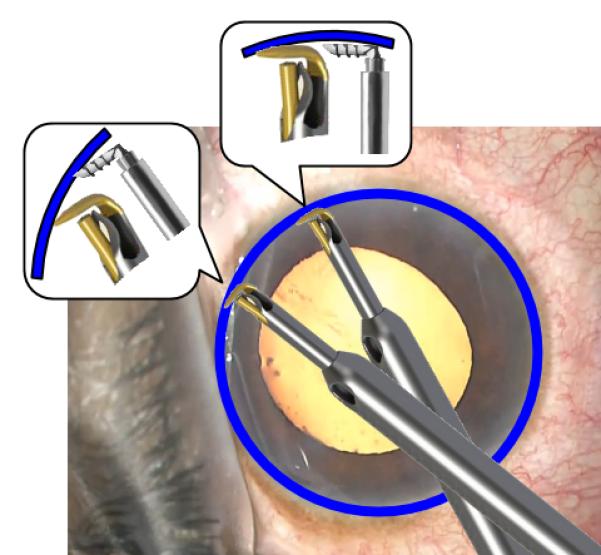
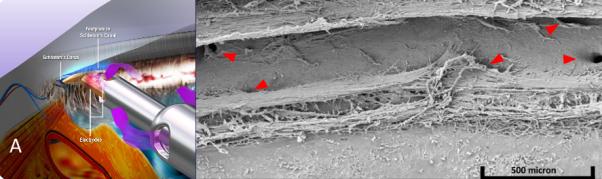
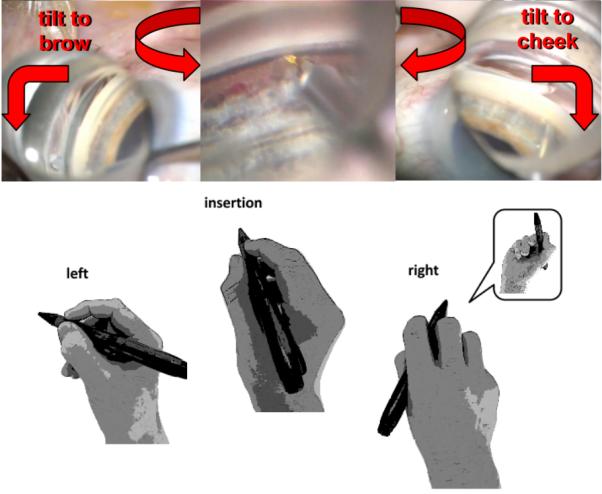
Minimally invasive glaucoma surgeries (MIGS) can improve the conventional, pressure-dependent outflow by bypassing or ablating the trabecular meshwork (TM), or creating alternative drainage routes into the suprachoroidal or subconjunctival space. They have a highly favourable risk profile compared to penetrating surgeries, and lower intraocular pressure with variable efficacy that may depend on the extent of outflow segments accessed. Since they are highly standardised procedures that use clear corneal incisions, they can elegantly be combined with cataract and refractive procedures to improve vision in the same session. There is a growing need for surgeons to become proficient in MIGS to address the increasing prevalence of glaucoma and cataracts in a well-informed, aging population. Techniques of visualisation and instrumentation in an anatomically highly confined space with semitransparent tissues are fundamentally different from other anterior segment surgeries, and present even experienced surgeons with a substantial learning curve. Here, we provide practical tips, and review techniques and outcomes of TM bypass and ablation MIGS.
Keywords: Angle; Glaucoma; Treatment Lasers; Treatment Surgery.
Figures

References
-
- Klaver CC, Wolfs RC, Vingerling JR, et al. Age-specific prevalence and causes of blindness and visual impairment in an older population: the Rotterdam Study. Arch Ophthalmol. 1998;116(5):653–8. - PubMed
-
- Shingleton BJ, Laul A, Nagao K, et al. Effect of phacoemulsification on intraocular pressure in eyes with pseudoexfoliation: single-surgeon series. J Cataract Refract Surg. 2008;34(11):1834–41. doi: 10.1016/j.jcrs.2008.07.025. - PubMed
-
- Huang G, Gonzalez E, Peng PH, et al. Anterior chamber depth, iridocorneal angle width, and intraocular pressure changes after phacoemulsification: narrow vs open iridocorneal angles. Arch Ophthalmol. 2011;129(10):1283–90. doi: 10.1001/archophthalmol.2011.272. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical