

Patients with microvascular obstruction after primary percutaneous coronary intervention show a gp91phox (NOX2) mediated persistent oxidative stress after reperfusion
- PMID: 24338297
- PMCID: PMC3821834
- DOI: 10.1177/2048872613504698
Patients with microvascular obstruction after primary percutaneous coronary intervention show a gp91phox (NOX2) mediated persistent oxidative stress after reperfusion
Abstract
Background: Persistent oxidative stress may play a key role in microvascular obstruction (MVO). We aimed at assessing the role of platelet gp91phox (NOX2), the catalytic subunit of NADPH oxidase in MVO.
Methods: We enrolled 40 patients with ST-elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention within 12 h from symptoms onset, either with angiographic MVO (n=20) or good angiographic myocardial reperfusion (MR) (n=20). Angiographic MVO was defined as a final thrombolysis in myocardial infarction (TIMI) flow ≤2 or TIMI flow of 3 with myocardial blush grade <2. NOX2 and isoprostanes (8-iso-PGF2α) levels, as assessed by enzyme-linked immunoadsorbent assay (ELISA) or by an enzyme immunoassays, respectively, were measured on admission, at 24 h and pre-discharge.
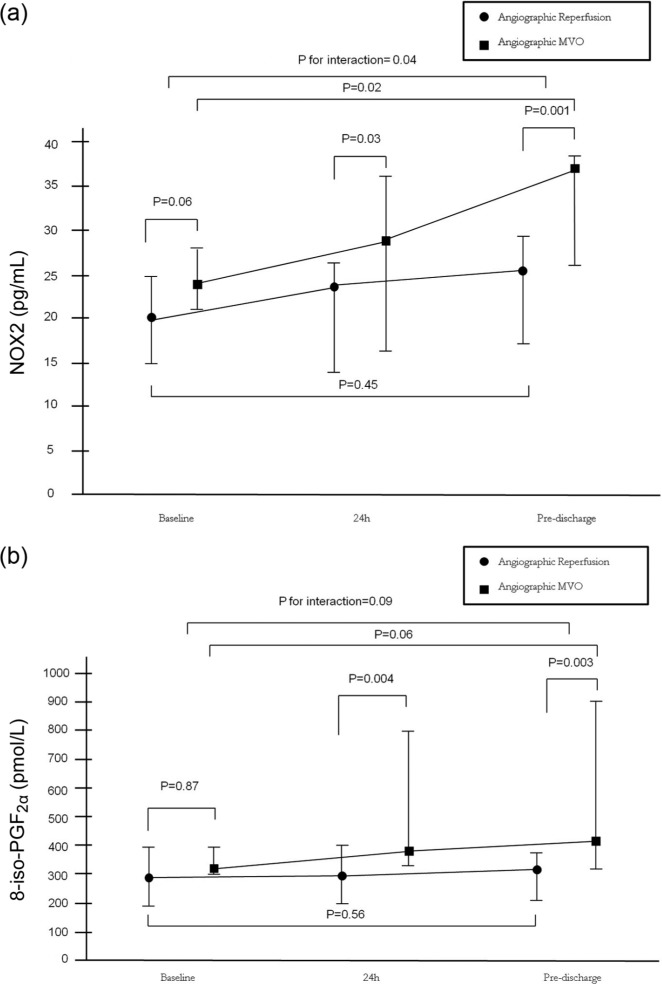
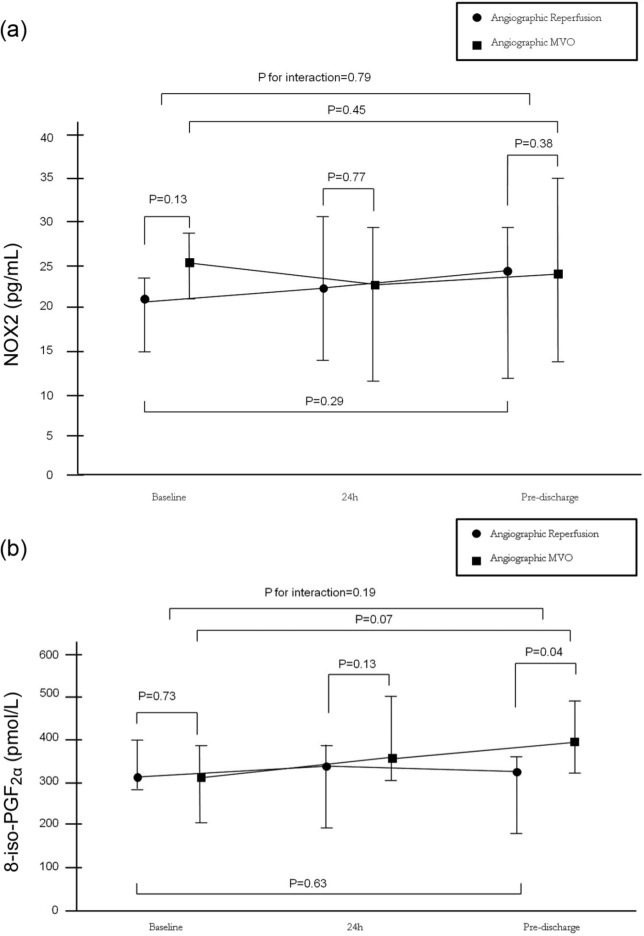
Results: NOX2 levels increased from baseline to pre-discharge in patients with angiographic MVO (20.25 (15-24.75) pg/ml vs 25.50 (17-29.25) pg/ml, p=0.02), but not in MR patients (p=0.45), with a significant interaction between baseline and pre-discharge levels among the two groups (p=0.04). The levels of 8-iso-PGF2α showed a trend to increase from baseline to pre-discharge in angiographic MVO patients (295 (183.50-389.25) pmol/l vs 322 (206-370) pmol/l, p=0.06), but not in patients with MR (p=0.56), with a trend for interaction between baseline and pre-discharge levels among the two groups (p=0.09).
Conclusion: Patients with MVO, but not those with myocardial reperfusion, have a sustained increase of NOX2 and 8-iso-PGF2α. Therapies targeting NOX2 or high dosage antioxidants should be tested for MVO prevention and treatment.
Keywords: ST-elevation myocardial infarction; microvascular obstruction; oxidative stress; primary percutaneous coronary intervention.
Conflict of interest statement
Figures
References
-
- Niccoli G, Burzotta F, Galiuto L, et al. Myocardial no-reflow in humans. J Am Coll Cardiol 2009; 54: 281–292 - PubMed
-
- Wu KC, Zerhouni EA, Judd RM, et al. Prognostic significance of microvascular obstruction by magnetic resonance imaging in patients with acute myocardial infarction. Circulation 1998; 97: 765–772 - PubMed
-
- Ito H. No-reflow phenomenon in patients with acute myocardial infarction: Its pathophysiology and clinical implications. Acta Med Okayama 2009; 63: 161–168 - PubMed
-
- Svilaas T, Vlaar PJ, van der Horst IC, et al. Thrombus aspiration during primary percutaneous coronary intervention. N Engl J Med 2008; 358: 557–567 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
