

Surgical versus endoscopic treatment of bile duct stones
- PMID: 24338858
- PMCID: PMC6464772
- DOI: 10.1002/14651858.CD003327.pub4
Surgical versus endoscopic treatment of bile duct stones
Abstract
Background: Between 10% to 18% of people undergoing cholecystectomy for gallstones have common bile duct stones. Treatment of the bile duct stones can be conducted as open cholecystectomy plus open common bile duct exploration or laparoscopic cholecystectomy plus laparoscopic common bile duct exploration (LC + LCBDE) versus pre- or post-cholecystectomy endoscopic retrograde cholangiopancreatography (ERCP) in two stages, usually combined with either sphincterotomy (commonest) or sphincteroplasty (papillary dilatation) for common bile duct clearance. The benefits and harms of the different approaches are not known.
Objectives: We aimed to systematically review the benefits and harms of different approaches to the management of common bile duct stones.
Search methods: We searched the Cochrane Hepato-Biliary Group Controlled Trials Register, Cochrane Central Register of Controlled Trials (CENTRAL, Issue 7 of 12, 2013) in The Cochrane Library, MEDLINE (1946 to August 2013), EMBASE (1974 to August 2013), and Science Citation Index Expanded (1900 to August 2013).
Selection criteria: We included all randomised clinical trials which compared the results from open surgery versus endoscopic clearance and laparoscopic surgery versus endoscopic clearance for common bile duct stones.
Data collection and analysis: Two review authors independently identified the trials for inclusion and independently extracted data. We calculated the odds ratio (OR) or mean difference (MD) with 95% confidence interval (CI) using both fixed-effect and random-effects models meta-analyses, performed with Review Manager 5.
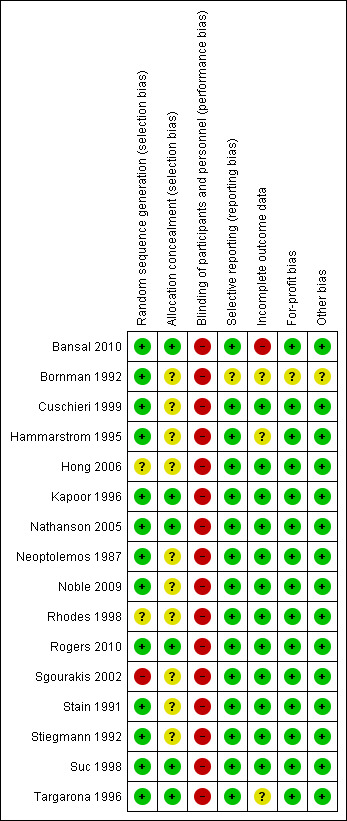
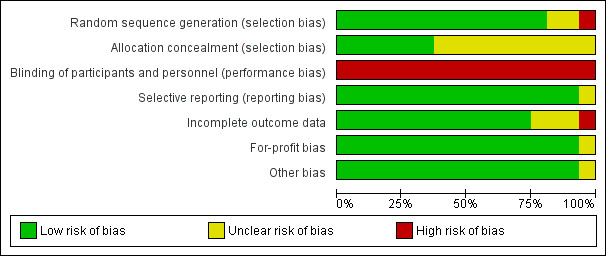
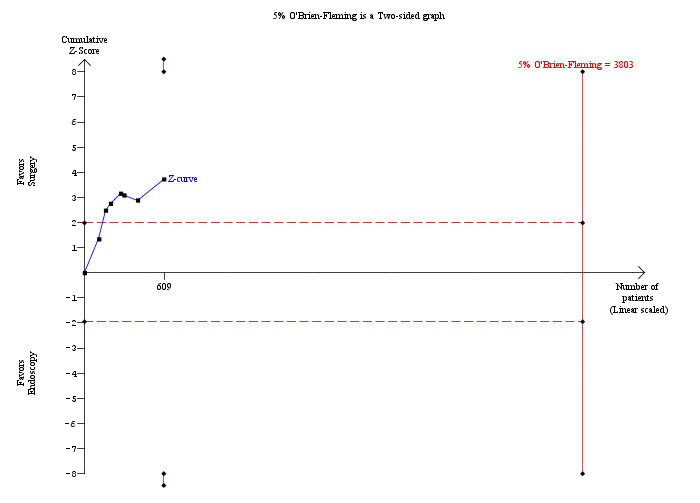
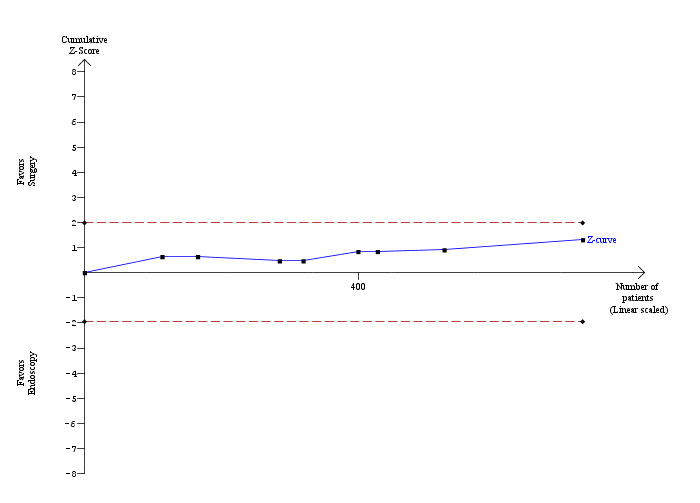
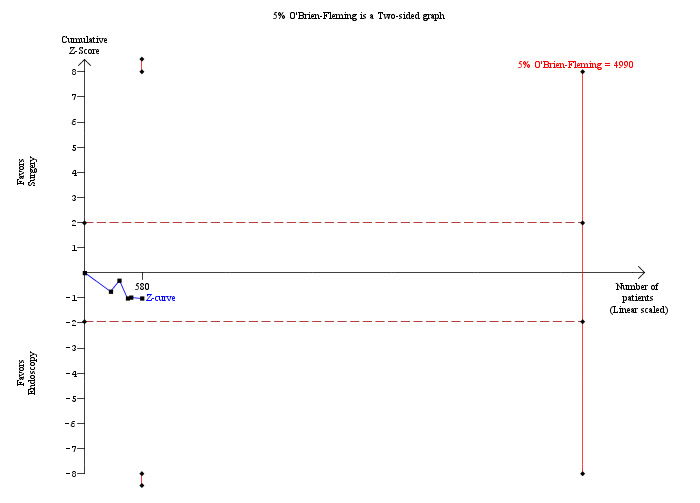
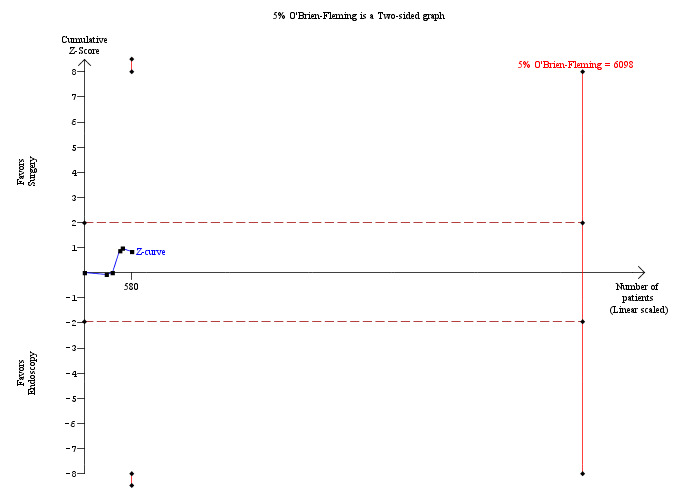
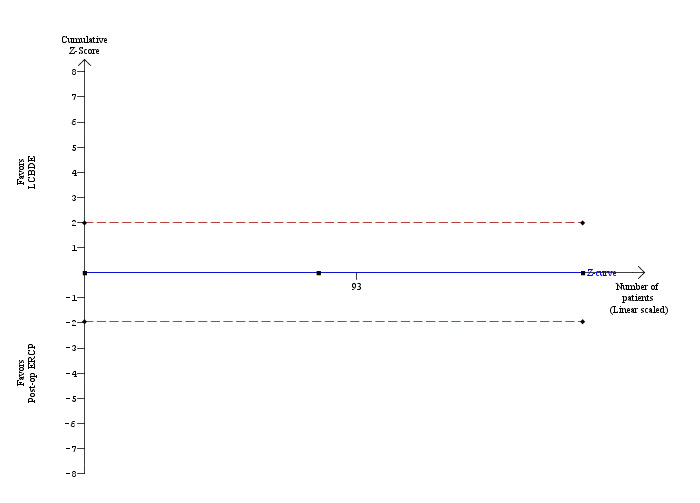
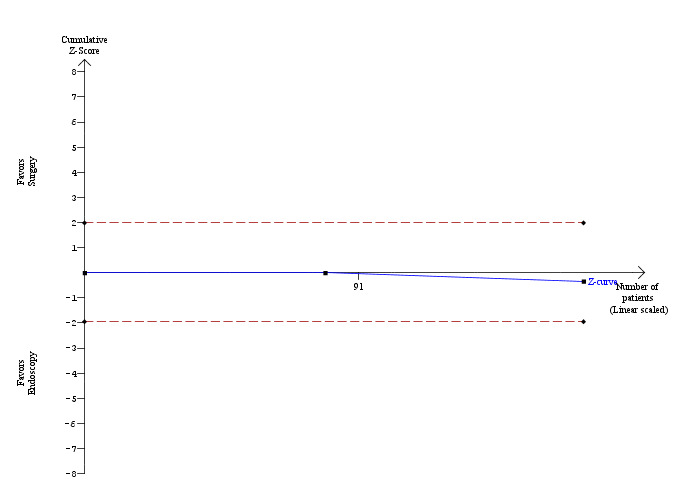
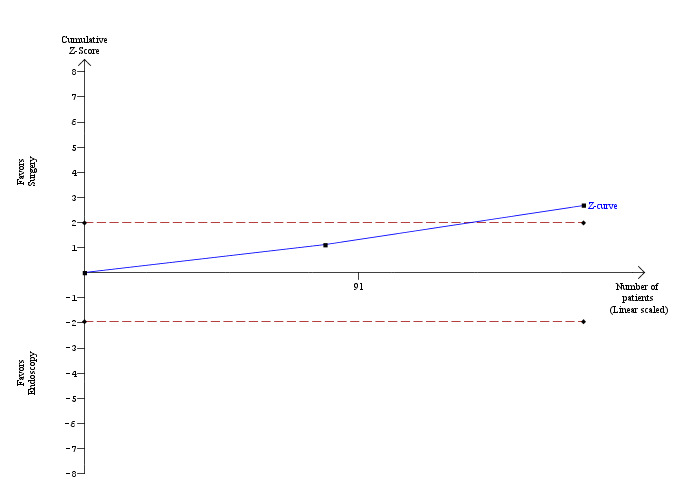
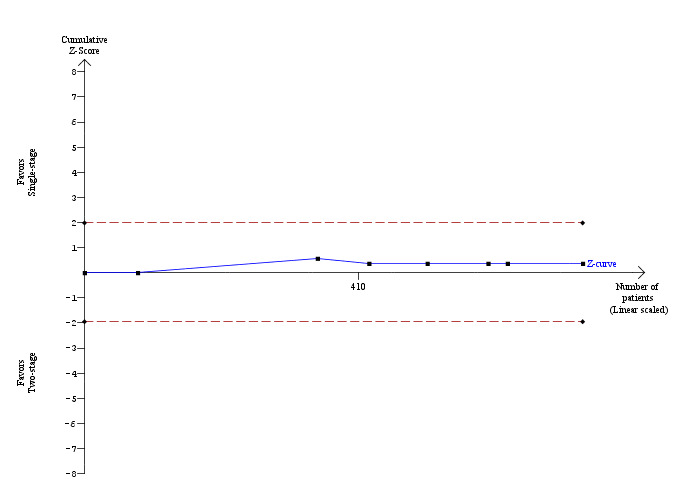
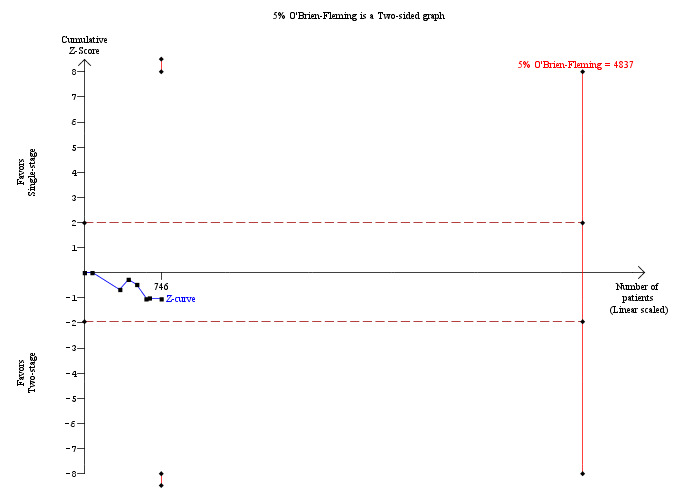
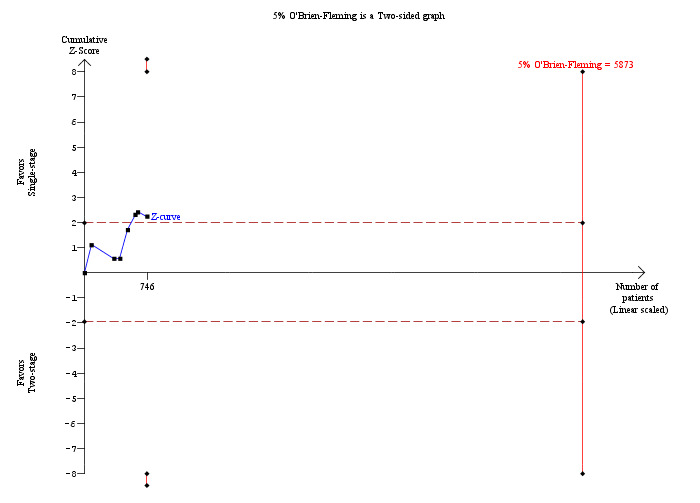
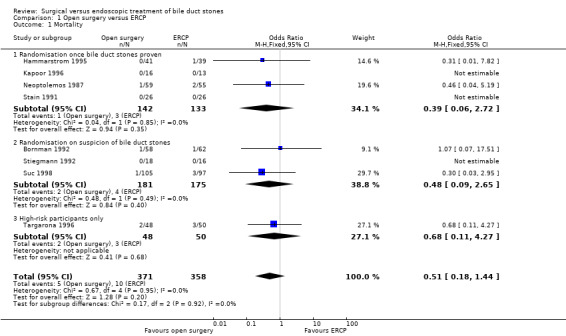
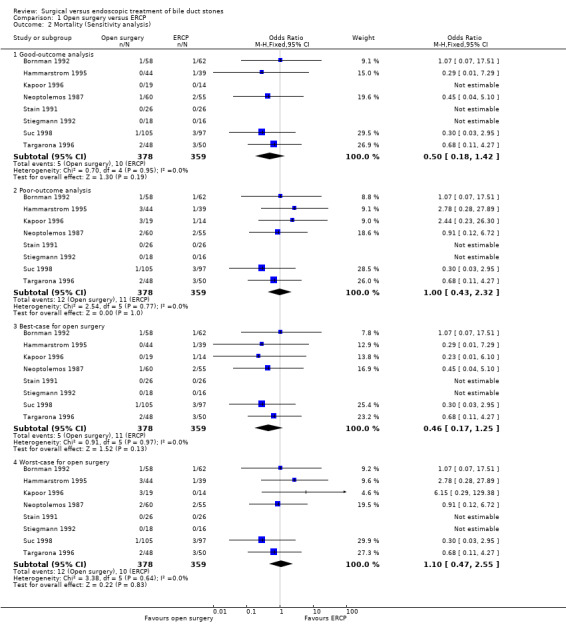
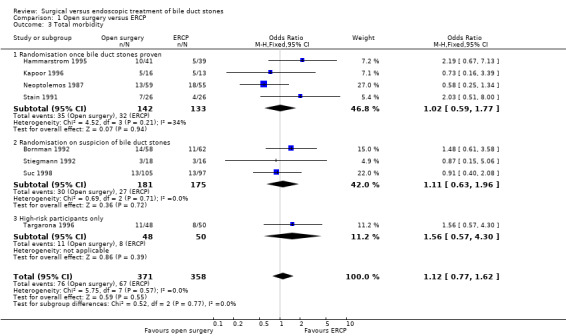
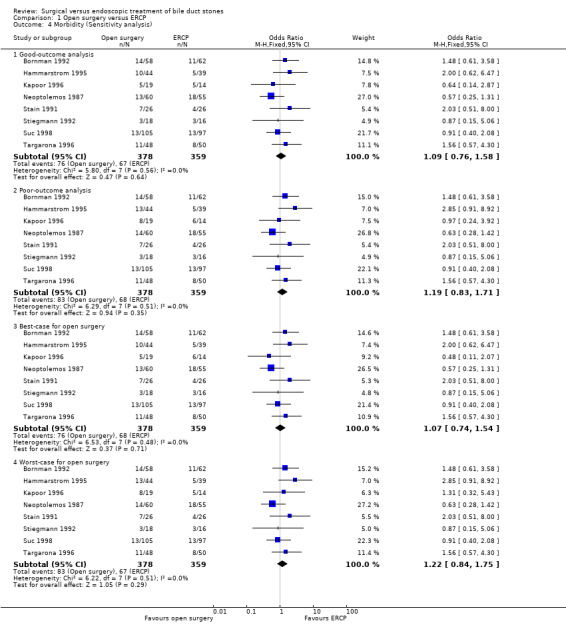
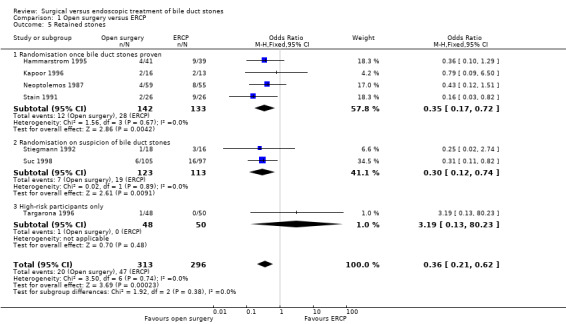
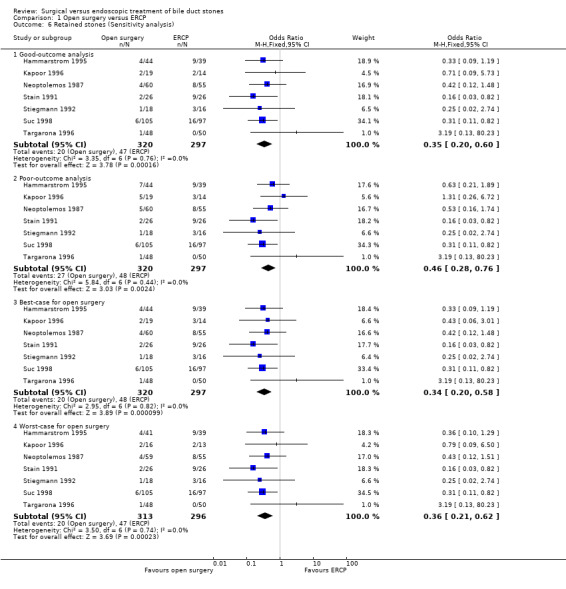
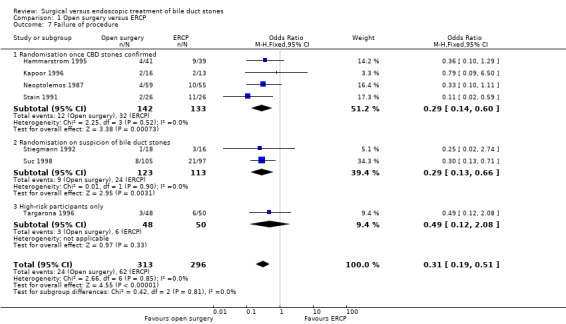
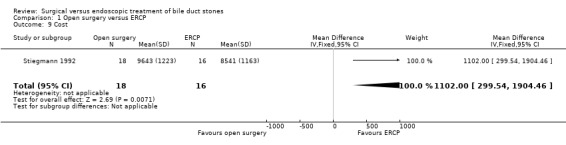
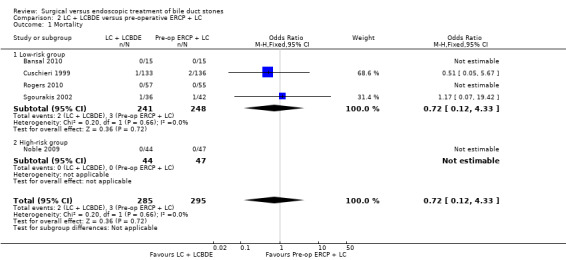
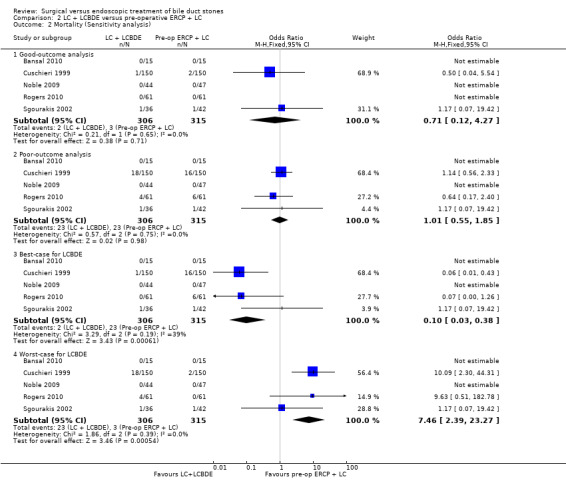
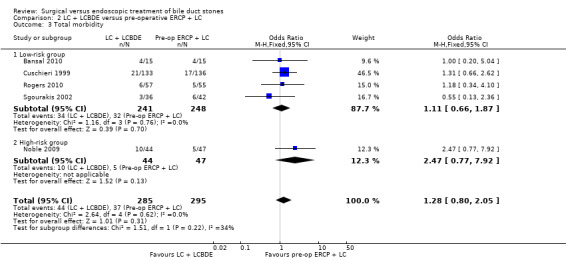
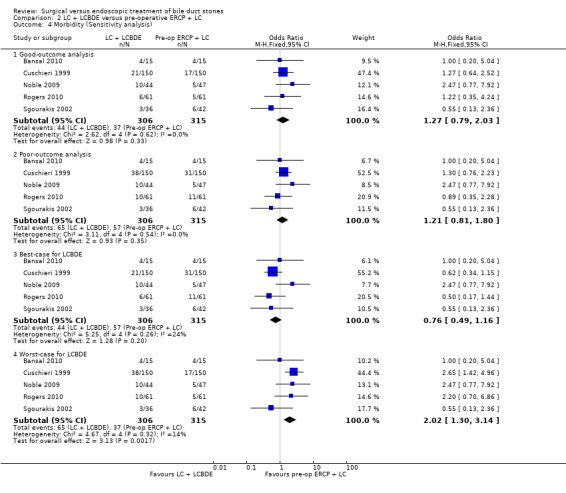
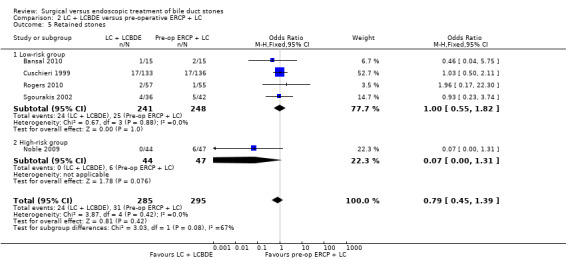
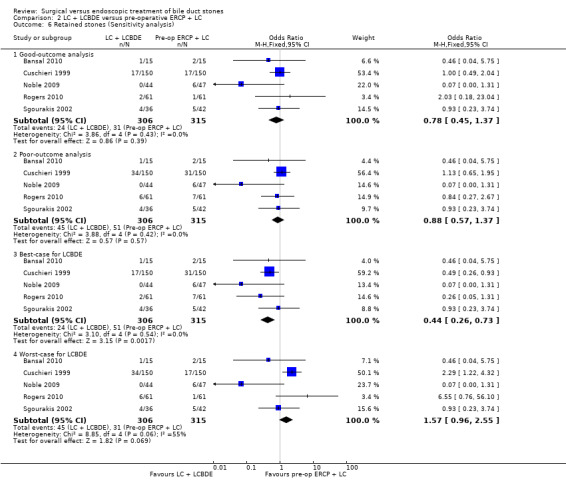
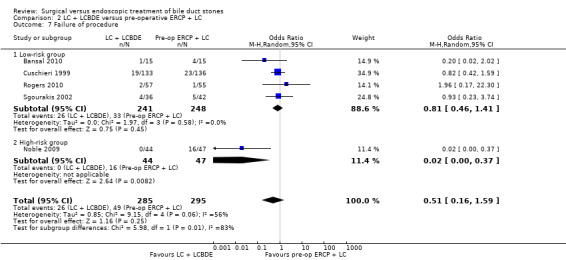
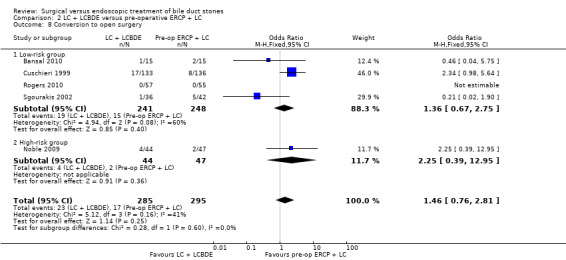
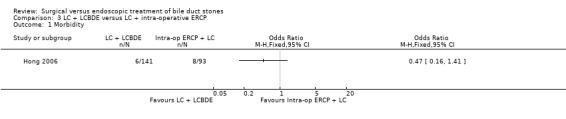
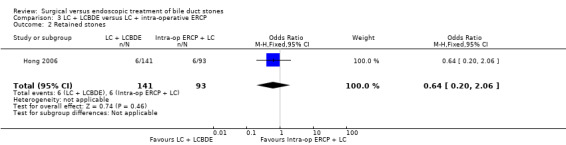
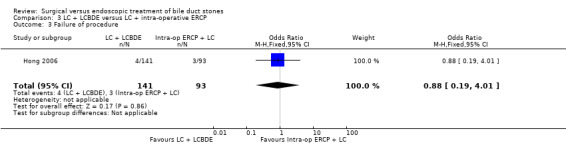
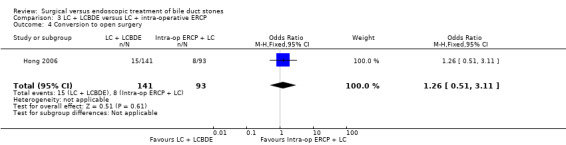
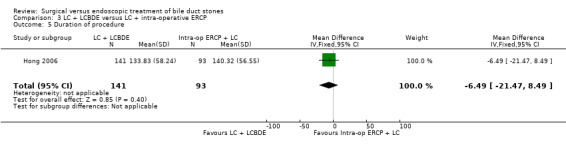
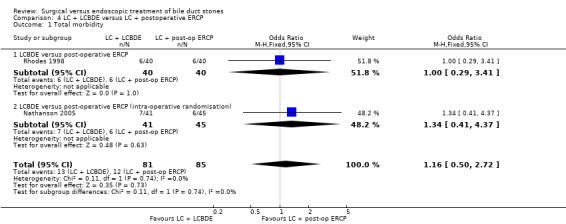
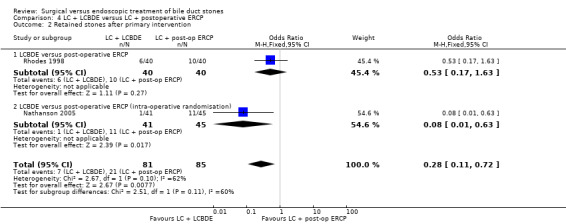
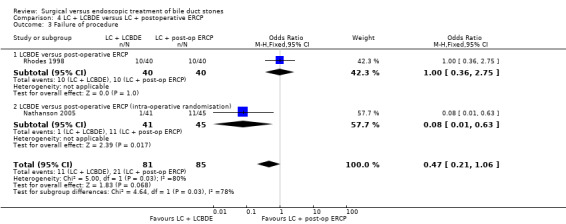
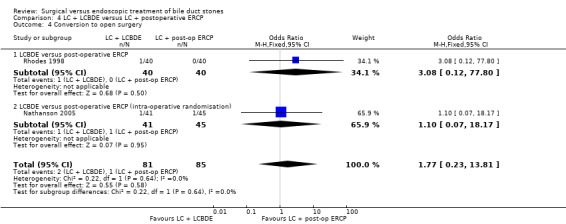
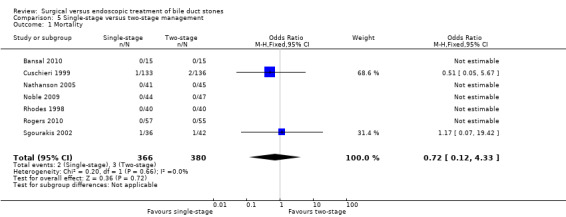
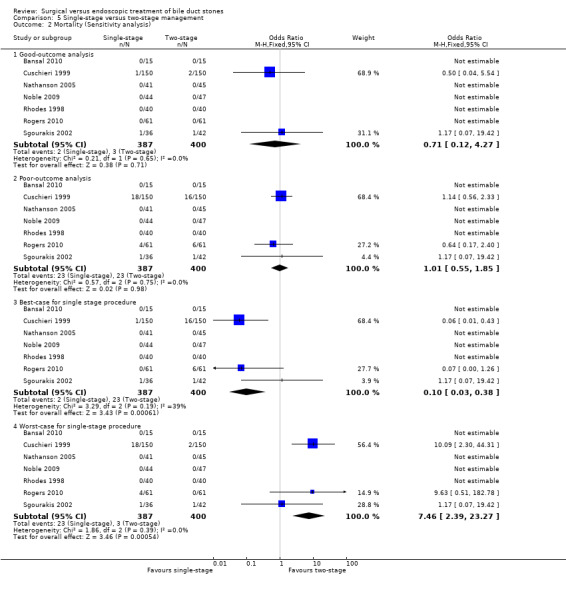
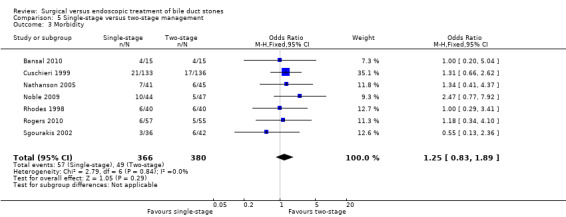
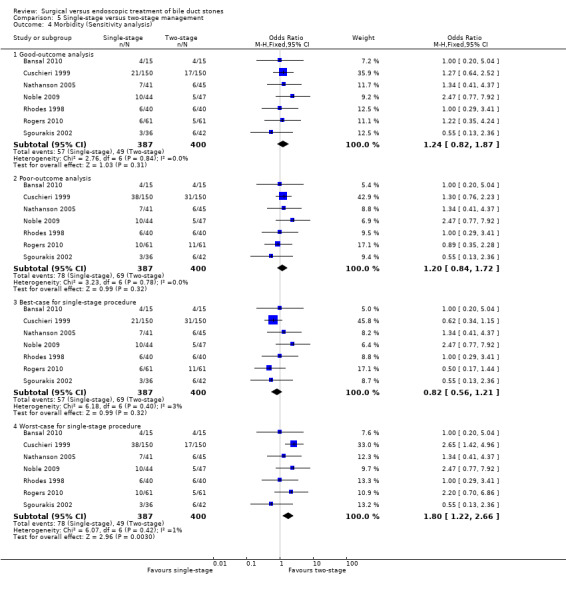
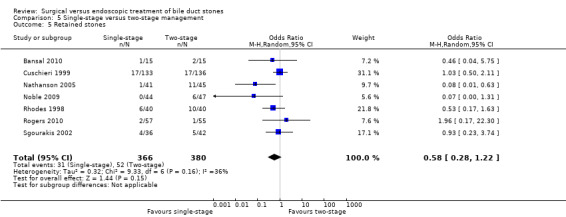
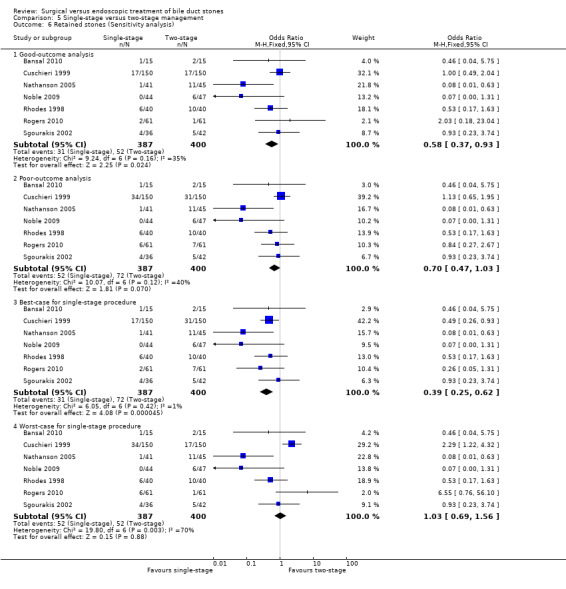
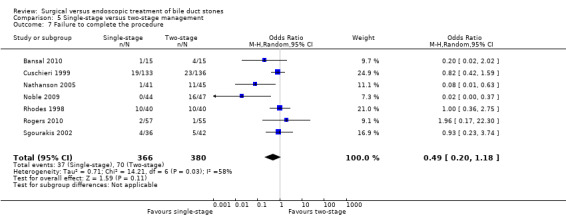
Main results: Sixteen randomised clinical trials with a total of 1758 randomised participants fulfilled the inclusion criteria of this review. Eight trials with 737 participants compared open surgical clearance with ERCP; five trials with 621 participants compared laparoscopic clearance with pre-operative ERCP; and two trials with 166 participants compared laparoscopic clearance with postoperative ERCP. One trial with 234 participants compared LCBDE with intra-operative ERCP. There were no trials of open or LCBDE versus ERCP in people without an intact gallbladder. All trials had a high risk of bias.There was no significant difference in the mortality between open surgery versus ERCP clearance (eight trials; 733 participants; 5/371 (1%) versus 10/358 (3%) OR 0.51;95% CI 0.18 to 1.44). Neither was there a significant difference in the morbidity between open surgery versus ERCP clearance (eight trials; 733 participants; 76/371 (20%) versus 67/358 (19%) OR 1.12; 95% CI 0.77 to 1.62). Participants in the open surgery group had significantly fewer retained stones compared with the ERCP group (seven trials; 609 participants; 20/313 (6%) versus 47/296 (16%) OR 0.36; 95% CI 0.21 to 0.62), P = 0.0002.There was no significant difference in the mortality between LC + LCBDE versus pre-operative ERCP +LC (five trials; 580 participants; 2/285 (0.7%) versus 3/295 (1%) OR 0.72; 95% CI 0.12 to 4.33). Neither was there was a significant difference in the morbidity between the two groups (five trials; 580 participants; 44/285 (15%) versus 37/295 (13%) OR 1.28; 95% CI 0.80 to 2.05). There was no significant difference between the two groups in the number of participants with retained stones (five trials; 580 participants; 24/285 (8%) versus 31/295 (11%) OR 0.79; 95% CI 0.45 to 1.39).There was only one trial assessing LC + LCBDE versus LC+intra-operative ERCP including 234 participants. There was no reported mortality in either of the groups. There was no significant difference in the morbidity, retained stones, procedure failure rates between the two intervention groups.Two trials assessed LC + LCBDE versus LC+post-operative ERCP. There was no reported mortality in either of the groups. There was no significant difference in the morbidity between laparoscopic surgery and postoperative ERCP groups (two trials; 166 participants; 13/81 (16%) versus 12/85 (14%) OR 1.16; 95% CI 0.50 to 2.72). There was a significant difference in the retained stones between laparoscopic surgery and postoperative ERCP groups (two trials; 166 participants; 7/81 (9%) versus 21/85 (25%) OR 0.28; 95% CI 0.11 to 0.72; P = 0.008.In total, seven trials including 746 participants compared single staged LC + LCBDE versus two-staged pre-operative ERCP + LC or LC + post-operative ERCP. There was no significant difference in the mortality between single and two-stage management (seven trials; 746 participants; 2/366 versus 3/380 OR 0.72; 95% CI 0.12 to 4.33). There was no a significant difference in the morbidity (seven trials; 746 participants; 57/366 (16%) versus 49/380 (13%) OR 1.25; 95% CI 0.83 to 1.89). There were significantly fewer retained stones in the single-stage group (31/366 participants; 8%) compared with the two-stage group (52/380 participants; 14%), but the difference was not statistically significantOR 0.59; 95% CI 0.37 to 0.94).There was no significant difference in the conversion rates of LCBDE to open surgery when compared with pre-operative, intra-operative, and postoperative ERCP groups. Meta-analysis of the outcomes duration of hospital stay, quality of life, and cost of the procedures could not be performed due to lack of data.
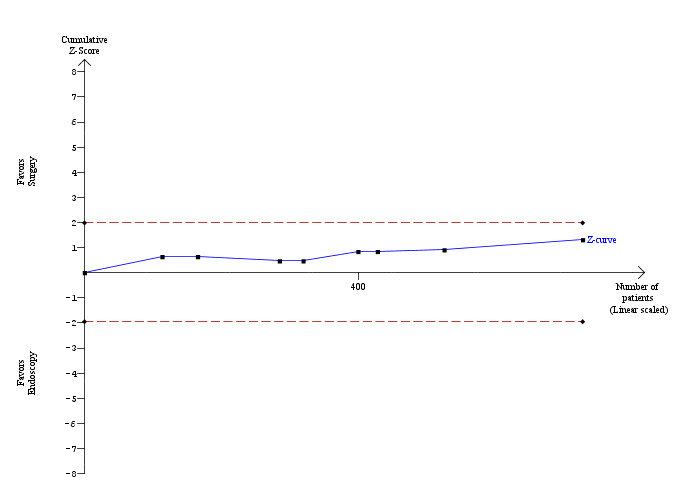
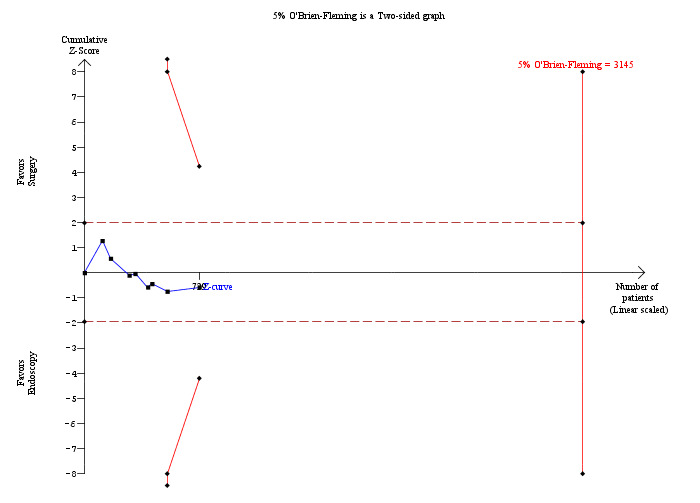
Authors' conclusions: Open bile duct surgery seems superior to ERCP in achieving common bile duct stone clearance based on the evidence available from the early endoscopy era. There is no significant difference in the mortality and morbidity between laparoscopic bile duct clearance and the endoscopic options. There is no significant reduction in the number of retained stones and failure rates in the laparoscopy groups compared with the pre-operative and intra-operative ERCP groups. There is no significant difference in the mortality, morbidity, retained stones, and failure rates between the single-stage laparoscopic bile duct clearance and two-stage endoscopic management. More randomised clinical trials without risks of systematic and random errors are necessary to confirm these findings.
Conflict of interest statement
None known.
Figures


Update of
-
Surgical versus endoscopic treatment of bile duct stones.Cochrane Database Syst Rev. 2013 Sep 3;(9):CD003327. doi: 10.1002/14651858.CD003327.pub3. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2013 Dec 12;(12):CD003327. doi: 10.1002/14651858.CD003327.pub4. PMID: 23999986 Updated.
References
References to studies included in this review
Bansal 2010 {published data only}
-
- Bansal VK, Misra MC, Garg P, Prabhu M. A prospective randomized trial comparing two‐stage versus single‐stage management of patients with gallstone disease and common bile duct stones. Surgical Endoscopy 2010;24:1986‐9. - PubMed
Bornman 1992 {unpublished data only}
-
- Bornman PC, Funnell IC, Wyk MEC, Krige JEJ, Graham S. Does ERCP before planned cholecystectomy benefit patients with suspected bile duct stones? A randomised trial [abstract]. South African Medical Journal 1991;81:41.
Cuschieri 1999 {published data only}
-
- Cuschieri A, Lezoche E, Mornino M, Croce E, Lacy A, Tooulo J, et al. E.A.E.S. multicenter prospective randomized trial comparing two‐stage vs single‐stage management of patients with gallstone disease and ductal calculi. Surgical Endoscopy 1999;13(10):952‐7. - PubMed
Hammarstrom 1995 {published data only}
-
- Hammarstrom LE, Holmin T, Stridbeck H, Ihse I. Long‐term follow‐up of a prospective randomized study of endoscopic versus surgical treatment of bile duct calculi in patients with gallbladder in situ. British Journal of Surgery 1995;82(11):1516‐21. - PubMed
Hong 2006 {published data only}
-
- Hong DF, Xin Y, Chen DW. Comparision of laparoscopic cholecystectomy combined with intraoperative endoscopic sphincterotomy and laparoscopic exploration of the common bile duct for cholecystocholedocholithiasis. Surgical Endoscopy 2006;20:424‐7. - PubMed
-
- Xin Y, Hong D, Cai X, Mou Y, Li L, Wang G, et al. Comparision of laparoscopic cholecystectomy combined with intraoperative endoscopic sphincterotomy and combined with laparoscopic common bile duct exploration in treatment of cholithiasis and calculus of common bile duct [Chinese]. National Medical Journal of China 2007;87(38):2703‐5. - PubMed
Kapoor 1996 {published data only}
Nathanson 2005 {published data only}
Neoptolemos 1987 {published data only}
Noble 2009 {published data only}
-
- Noble H, Tranter S, Chesworth T, Norton S, Thompson MD. A randomized, clinical trial to compare endoscopic sphincterotomy and subsequent laparoscopic cholecystectomy with primary laparoscopic bile duct exploration during cholecystectomy in higher risk patients with choledocholithiasis. Journal of Laparoendoscopic and Advanced Surgical Techniques 2009;19(6):713‐20. - PubMed
Rhodes 1998 {published data only}
-
- Rhodes M, Sussman L, Cohen L, Lewis MP. Randomised trial of laparoscopic exploration of common bile duct versus postoperative endoscopic retrograde cholangiography for common bile duct stones. Lancet 1998;351(9097):159‐61. - PubMed
Rogers 2010 {published data only}
-
- Rogers S, Cello JP, Horn JK, Siperstein A, Campbell A, Mackersie R, et al. Randomized controlled clinical trial of laparascopic cholecystectomy plus laparoscopic common bile duct exploration (LC+LCBDE) vs ERCP sphincterotomy plus laparascopic cholecystectomy (ERCP/S+LC) for common bile duct stone disease [abstract]. Journal of Gastroenterology and Hepatology 1999;14(Suppl):S110.
-
- Rogers SJ, Cello JP, Horn JK, Siperstein AE, Schecter WP, Campbell AR, et al. Prospective randomised trial of LC+LCBDE vs ERCP/S+LC for common bile duct stone disease. Archives of Surgery 2010;145(1):28‐33. - PubMed
Sgourakis 2002 {published data only}
-
- Sgourakis G, Karaliotas K. Laparoscopic common bile duct exploration and cholecystectomy versus endoscopic stone extraction and laparoscopic cholecystectomy for choledocholithiasis. A prospective randomized study. Minerva Chirurgica 2002;57(4):467‐74. - PubMed
Stain 1991 {published data only}
Stiegmann 1992 {published data only}
-
- Stiegmann GV, Goff JS, Mansour A, Pearlman N, Reveille RM, Norton L. Precholecystectomy endoscopic cholangiography and stone removal is not superior to cholecystectomy, cholangiography, and common duct exploration. American Journal of Surgery 1992;163(2):227‐30. - PubMed
Suc 1998 {published data only}
-
- Suc B, Escat J, Cherqui D, Fourtanier G, Hay JM, Fingerhut A, et al. Surgery vs endoscopy as primary treatment in symptomatic patients with suspected common bile duct stones: a multicenter randomized trial. French Associations for Surgical Research. Archives of Surgery 1998;133(7):702‐8. - PubMed
Targarona 1996 {published data only}
-
- Targarona EM, Perez Ayuso RM, Bordas JM, Ros E, Pros I, Martinez J, et al. Randomised trial of endoscopic sphincterotomy with gall bladder left in situ versus open surgery for common bile duct calculi in high risk patients. Lancet 1996;347:926‐9. - PubMed
References to studies excluded from this review
Airan 1992 {published data only}
-
- Airan M, Appel M, Berci G, Coburg AJ, Cohen M, Cuschieri A, et al. Retrospective and prospective multi‐institutional laparoscopic cholecystectomy study organized by the Society of American Gastrointestinal Endoscopic Surgeons. Surgical Endoscopy 1992;6(4):169‐78. - PubMed
Ammori 2000 {published data only}
-
- Ammori BJ, Birbas K, Davides D, Vezakis A, Larvin M, McMahon MJ. Routine vs "on demand" postoperative ERCP for small bile duct calculi detected at intraoperative cholangiography. Clinical evaluation and cost analysis. Surgical Endoscopy 2000;14(12):1123‐6. - PubMed
Andreasen 1998 {published data only}
-
- Andreasen DA, Larsen JF. ERCP and laparoscopic cholecystectomy [ERCP og laparoskopisk kolecystektomi]. Ugeskrift for Laeger 1998;160(32):4626‐9. - PubMed
Berci 1994 {published data only}
-
- Berci G, Morgenstern L. Laparoscopic management of common bile duct stones. A multi‐institutional SAGES study. Society of American Gastrointestinal Endoscopic Surgeons. Surgical Endoscopy 1994;8(10):1168‐75. - PubMed
Bergamaschi 1999 {published data only}
-
- Bergamaschi R, Tuech JJ, Braconier L, Walsoe HK, Marvik R, Boyet J, et al. Selective endoscopic retrograde cholangiography prior to laparoscopic cholecystectomy for gallstones. American Journal of Surgery 1999;178(1):46‐9. - PubMed
Boeckl 1988 {published data only}
-
- Boeckl O, Heinerman M, Pimpl W. Influence of preoperative selective endoscopy on the results and treatment concept of bile duct surgery [Einfluss der praoperativen selektiven Endoskopie auf Resultate und Therapiekonzept der Gallengangschirurgie]. Deutsche Medizinische Wochenschrift 1988;113(50):1950‐5. - PubMed
Boerma 2002 {published data only}
-
- Boerma D, Rauws EA, Keulemans YC, Janssen IM, Bolwerk CJ, Timmer R, et al. Wait‐and‐see policy or laparoscopic cholecystectomy after endoscopic sphincterotomy for bile‐duct stones: a randomised trial. Lancet 2002;360:761‐5. - PubMed
Bonatsos 1996 {published data only}
-
- Bonatsos G, Leandros E, Polydorou A, Romanos A, Dourakis N, Birbas C, et al. ERCP in association with laparoscopic cholecystectomy. A strategy to minimize the number of unnecessary ERCPs. Surgical Endoscopy 1996;10(1):37‐40. - PubMed
Budzynski 1997 {published data only}
-
- Budzynski A, Bobrzynski A, Rembiasz K, Biesiada Z, Dutkiewicz W. The problem of common bile duct calculi in the era of laparoscopic cholecystectomy [Problem kamicy przewodowej w dobie cholecystektomii laparoskopowej]. Wiadomosci Lekarskie 1997;50(Suppl 1 Pt 1):235‐8. - PubMed
Cemachovic 2000 {published data only}
-
- Cemachovic I, Letard JC, Begin GF, Rousseau D, Nivet JM. Intraoperative endoscopic sphincterotomy is a reasonable option for complete single‐stage minimally invasive biliary stones treatment: short‐term experience with 57 patients. Endoscopy 2000;32(12):956‐62. - PubMed
Chan 1996 {published data only}
-
- Chan AC, Chung SC, Wyman A, Kwong KH, Ng EK, Lau JY, et al. Selective use of preoperative endoscopic retrograde cholangiopancreatography in laparoscopic cholecystectomy. Gastrointestinal Endoscopy 1996;43(3):212‐5. - PubMed
Chang 2000 {published data only}
Cisek 1994 {published data only}
-
- Cisek PL, Greaney GC. The role of endoscopic retrograde cholangiopancreatography with laparoscopic cholecystectomy in the management of choledocholithiasis. American Surgeon 1994;60(10):772‐6. - PubMed
Conigliaro 1995 {published data only}
-
- Conigliaro R, Ricci E, Sassatelli R, Pacchione D, Bertoni G, Mortilla MG, et al. Common bile duct stones and cholecystectomy: a prospective multicentric study comparing different treatments. Giornale Italiano di Endoscopia Digestiva 1995;18(4):237‐45.
Coppola 1996 {published data only}
-
- Coppola R, D'Ugo D, Ciletti S, Riccioni ME, Cosentino L, Magistrelli P, et al. ERCP in the era of laparoscopic biliary surgery. Experience with 407 patients. Surgical Endoscopy 1996;10(4):403‐6. - PubMed
Daradkeh 2000 {published data only}
-
- Daradkeh S, Shennak M, Abu‐Khalaf M. Selective use of perioperative ERCP in patients undergoing laparoscopic cholecystectomy. Hepato‐Gastroenterology 2000;47(35):1213‐5. - PubMed
Davis 1997 {published data only}
-
- Davis WZ, Cotton PB, Arias R, Williams D, Onken JE. ERCP and sphincterotomy in the context of laparoscopic cholecystectomy: academic and community practice patterns and results. American Journal of Gastroenterology 1997;92(4):597‐601. - PubMed
Decker 2003 {published data only}
-
- Decker G, Borie F, Millat B, Berthou JC, Deleuze A, Drouard F, et al. One hundred laparoscopic choledochotomies with primary closure of the common bile duct. Surgical Endoscopy 2003;17(1):12‐8. - PubMed
Dias 2002 {published data only}
-
- Dias MM, Martin CJ, Cox MR. Pattern of management of common bile duct stones in the laparoscopic era: a NSW survey. Australian and New Zealand Journal of Surgery 2002;72(3):181‐5. - PubMed
Drouard 1995 {published data only}
-
- Drouard F, Passone‐Szerzyna N, Berthou JC. Laparoscopic treatment of common bile duct calculi [Traitement laparoscopique de la lithiase de la voie biliaire principale]. Annales de Chirurgie 1995;49(7):596‐601. - PubMed
Drouard 1997 {published data only}
-
- Drouard F, Passone‐Szerzyna N, Berthou JC. Laparoscopic treatment of common bile duct stones. Hepato‐Gastroenterology 1997;44(13):16‐21. - PubMed
Ebner 2004 {published data only}
-
- Ebner S, Rechner J, Beller S, Erhart K, Riegler FM, Szinicz G. Laparoscopic management of common bile duct stones. Surgical Endoscopy and Other Interventional Techniques 2004;18(5):762‐5. - PubMed
El Geidie 2011 {published data only}
-
- Geidie AA, Ebidy GK, Naeem YM. Preoperative versus intraoperative endoscopic sphincterotomy for management of common bile duct stones. Surgical Endoscopy 2011;25:1230‐7. - PubMed
Fanning 1997 {published data only}
-
- Fanning NF, Horgan PG, Keane FBV. Evolving management of common bile duct stones in the laparoscopic era. Journal of the Royal College of Surgeons of Edinburgh 1997;42:389‐94. - PubMed
Frazee 1993 {published data only}
-
- Frazee RC, Roberts J, Symmonds R, Hendricks JC, Snyder S, Smith R, et al. Combined laparoscopic and endoscopic management of cholelithiasis and choledocholithiasis. American Journal of Surgery 1993;166(6):702‐6. - PubMed
Galloway 1994 {published data only}
-
- Galloway SW, Blazeby J, Tulloh B, Poskitt KR. Combined laparoscopic and endoscopic treatment of gallstones and bile duct stones: a prospective study. British Journal of Surgery 1994;81(11):1699‐70. - PubMed
Giurgiu 1999 {published data only}
-
- Giurgiu DI, Margulies DR, Carroll BJ, Gabbay J, Iida A, Takagi S, et al. Laparoscopic common bile duct exploration: long‐term outcome. Archives of Surgery 1999;134(8):839‐44. - PubMed
Gonzalez 1989 {published data only}
-
- Gonzalez JC, Gomis J, Zoghbi S, Capozzolo N, Aldana K, Nino M, et al. Preoperative endoscopic sphincterotomy [Esfinterotomia endoscopica preoperatoria]. Genetic Engineering News 1989;43(4):247‐50. - PubMed
Hamy 2003 {published data only}
-
- Hamy A, Hennekinne S, Pessaux P, Lada P, Randriamananjo S, Lermite E, et al. Endoscopic sphincterotomy prior to laparoscopic cholecystectomy for the treatment of cholelithiasis. Surgical Endoscopy 2003;17:872‐5. - PubMed
Heili 1999 {published data only}
-
- Heili M, Wintz NK, Fowler DL. Choledocholithiasis: endoscopic versus laparoscopic management. American Surgeon 1999;2:135‐8. - PubMed
Heinerman 1989 {published data only}
Hoyuela 1999 {published data only}
-
- Hoyuela C, Cugat E, Bretcha P, Collera P, Espinos J, Marco C. Must ERCP be routinely performed if choledocholithiasis is suspected?. Digestive Surgery 1999;16(5):411‐4. - PubMed
Hui 2002 {published data only}
Huynh 1996 {published data only}
-
- Huynh CH, Stadt J, Deviere J, Mehdi A, Nakadi I, Cremer M, et al. Preoperative endoscopic retrograde cholangiopancreatography: therapeutic impact in a general population of patients needing a cholecystectomy. Hepato‐Gastroenterology 1996;43(12):1484‐91. - PubMed
Kapoor 1994 {published data only}
-
- Kapoor R, Pradeep R, Sikora SS, Saxena R, Kapoor VK, Kaushik SP. Appraisal of surgical and endoscopic management of choledocholithiasis. Australian and New Zealand Journal of Surgery 1994;64(9):599‐603. - PubMed
Khuroo 1989 {published data only}
-
- Khuroo MS, Mahajan R, Zargar SA, Javid G, Banday M. Endoscopic vs surgical drainage of biliary tract in acute pyogenic cholangitis: a controlled study. Indian Journal of Gastroenterology 1989;8(2):119. - PubMed
Kullman 1996 {published data only}
-
- Kullman E, Borch K, Lindstrom E, Svanvik J, Anderberg B. Management of bile duct stones in the era of laparoscopic cholecystectomy: appraisal of routine operative cholangiography and endoscopic treatment. European Journal of Surgery 1996;162(11):873‐80. - PubMed
Lai 1992 {published data only}
-
- Lai EC, Mok FP, Tan ES, Lo CM, Fan ST, You KT, et al. Endoscopic biliary drainage for severe acute cholangitis. New England Journal of Medicine 1992;326(24):1582‐6. - PubMed
Lella 2006 {published data only}
-
- Lella F, Bagnolo F, Rebuffat C, Scalambra M, Bonassi U, Colombo E. Use of the laparoscopic‐endoscopic approach, the so‐called "rendezvous" technique, in cholecystocholedocholithiasis. Surgical Endoscopy 2006;20:419‐23. - PubMed
Lezoche 1996 {published data only}
-
- Lezoche E, Paganini AM, Carlei F, Feliciotti F, Lomanto D, Guerrieri M. Laparoscopic treatment of gallbladder and common bile duct stones: a prospective study. World Journal of Surgery 1996;20(5):535‐41. - PubMed
Lezoche 2000 {published data only}
-
- Lezoche E, Paganini AM. Technical considerations and laparoscopic bile duct exploration: transcystic and choledochotomy. Seminars in Laparoscopic Surgery 2000;7(4):262‐78. - PubMed
Liberman 1996 {published data only}
-
- Liberman MA, Phillips EH, Carroll BJ, Fallas MJ, Rosenthal R, Hiatt J. Cost‐effective management of complicated choledocholithiasis: laparoscopic transcystic duct exploration or endoscopic sphincterotomy. Journal of the American College of Surgeons 1996;182:488‐94. - PubMed
Liu 1996 {published data only}
-
- Liu CL, Lai EC, Lo CM, Chu KM, Fan ST, Wong J. Combined laparoscopic and endoscopic approach in patients with cholelithiasis and choledocholithiasis. Surgery 1996;119(5):534‐7. - PubMed
Magnanini 1994 {published data only}
-
- Magnanini F, Peralta C, Pardo R, Curras A, Zalar A, Olmos M. Endoscopic retrograde cholangiopancreatography: before and after laparoscopic cholecystectomy. Acta Gastroenterologica Latinoamericana 1994;24(4):213‐7. - PubMed
Martin 1998 {published data only}
Martin 2002 {published data only}
-
- Martin CJ, Cox MR, Vaccaro L. Laparoscopic transcystic bile duct stenting in the management of common bile duct stones. Australian and New Zealand Journal of Surgery 2002;72(4):258‐64. - PubMed
Masci 1999 {published data only}
-
- Masci E, Fanti L, Mariani A, Guerini S, Zuliani W, Baccari P, et al. Selection criteria for pre‐operative endoscopic retrograde cholangiography and endoscopic‐laparoscopic treatment of biliary stones. European Journal of Gastroenterology & Hepatology 1999;11(7):781‐4. - PubMed
Materia 1996 {published data only}
-
- Materia A, Pizzuto G, Silecchia G, Fiocca F, Fantini A, Spaziani E, et al. Sequential endoscopic‐laparoscopic treatment of cholecystocholedocholithiasis. Surgical Laparoscopy, Endoscopy & Percutaneous Techniques 1996;6(4):273‐7. - PubMed
Meyer 1999 {published data only}
-
- Meyer C, Le JV, Rohr S, Thiry LC, Bourtoul C, Duclos B, et al. Management of common bile duct stones by laparoscopic cholecystectomy and endoscopic sphincterotomy: pre‐, per‐ or postoperative sphincterotomy?. Digestive Surgery 1999;16(1):26‐31. - PubMed
Meyer 2002 {published data only}
-
- Meyer C, Le JV, Rohr S, Duclos B, Reimund JM, Baumann R. Management of common bile duct stones in a single operation combining laparoscopic cholecystectomy and peroperative endoscopic sphincterotomy. Journal of Hepato‐Biliary‐Pancreatic Surgery 2002;9(2):196‐200. - PubMed
Michel 2000 {published data only}
-
- Michel J, Navarro F, Montpeyroux F, Burgel JS, Moine MC, Daures JP, et al. Treatment of common bile duct stones with laparoscopy. Retrospective multicenter study with 612 patients [Traitement de la lithiase de la voie biliaire principale sous laparoscopie. Etude retrospective multicentrique chez 612 malades]. Gastroenterologie Clinique et Biologique 2000;24(4):404‐8. - PubMed
Mijal 1997 {published data only}
-
- Mijal M, Ciechanski A, Chmurzynski M, Zinkiewicz K, Cwik G, Misiuna P. Comparison of combined (endoscopic sphincterotomy + laparoscopic cholecystectomy) and classical treatment of obstructive jaundice in the course of cholelithiasis [Porownanie wynikow skojarzonego (ES + ChL) i klasycznego leczenia zoltaczki mechanicznej w przebiegu kamicy zolciowej]. Wiadomosci Lekarskie 1997;50(Suppl 1 Pt 1):242‐5. - PubMed
Millat 1995 {published data only}
-
- Millat B, Fingerhut A, Deleuze A, Briandet H, Marrel E, Seguin C, et al. Prospective evaluation in 121 consecutive unselected patients undergoing laparoscopic treatment of choledocholithiasis. British Journal of Surgery 1995;82(9):1266‐9. - PubMed
Millat 1996 {published data only}
-
- Millat B, Deleuze A, Atger J, Briandet H, Fingerhut A, Marrel E, et al. Treatment of common bile duct lithiasis under laparoscopy. A prospective multicenter study in 189 patients [Traitement de la lithiase de la voie biliaire principale sous laparoscopie]. Gastroenterologie Clinique et Biologique 1996;20(4):339‐45. - PubMed
Millat 1997 {published data only}
-
- Millat B, Atger J, Deleuze A, Briandet H, Fingerhut A, Guillon F, et al. Laparoscopic treatment for choledocholithiasis: a prospective evaluation in 247 consecutive unselected patients. Hepato‐Gastroenterology 1997;44(13):28‐34. - PubMed
Miller 1988 {published data only}
Mo 2002 {published data only}
-
- Mo LR, Chang KK, Wang CH, Yau MP, Yang TM. Preoperative endoscopic sphincterotomy in the treatment of patients with cholecystocholedocholithiasis. Journal of Hepato‐Biliary‐Pancreatic Surgery 2002;9(2):191‐5. - PubMed
Moreaux 1995 {published data only}
-
- Moreaux J. Traditional surgical management of common bile duct stones: a prospective study during a 20‐year experience. American Journal of Surgery 1995;169(2):220‐6. - PubMed
Morino 2006 {published data only}
Neoptolemos 89 {published data only}
Neuhaus 1992 {published data only}
-
- Neuhaus H, Ungeheuer A, Feussner H, Classen M, Siewert JR. Laparoscopic cholecystectomy: ERCP as standard preoperative diagnostic technique [Laparoskopische Cholezystektomie: ERCP als preoperative Standarddiagnostik?]. Deutsche Medizinische Wochenschrift 1992;117(49):1863‐7. - PubMed
Niu 1995 {published data only}
-
- Niu J, Shou NH, Forbes JF, Sun XY, Hu SY, Liu FJ. Laparoscopic exploration of intra‐ and extrahepatic bile ducts and T‐tube drainage. Australian and New Zealand Journal of Surgery 1995;65(3):189‐93. - PubMed
Paganini 1998 {published data only}
-
- Paganini AM, Lezoche E. Follow‐up of 161 unselected consecutive patients treated laparoscopically for common bile duct stones. Surgical Endoscopy 1998;12(1):23‐9. - PubMed
Palacios‐Macedo 1995 {published data only}
-
- Palacios‐Macedo A, Herrera MF, Moran MA, Gonzalez Garcia M, Chan Nunez C, Hernandez‐Ortiz J. Endoscopy and laparoscopy in the treatment of lithiasic cholecystitis associated with benign bile duct obstruction [Endoscopia y laparoscopia en el tratamiento de la colecistitis litiasica asociada a obstruccion benigna de via biliar]. Revista de Investigacion Clinica 1995;47(2):103‐7. - PubMed
Pedersen 1998 {published data only}
-
- Pedersen FM, Brandt CJ, Schaffalitzky de Muckadell OB. Choledocholithiasis. Endoscopic treatment of 416 consecutive patients [Choledocholitiasis. Endoskopisk behandling af 416 konsekutive patienter]. Ugeskrift for Laeger 1998;160(45):6526‐9. - PubMed
Pereira‐Lima 2001 {published data only}
-
- Pereira‐Lima JC, Rynkowski CB, Rhoden EL. Endoscopic treatment of choledocholithiasis in the era of laparoscopic cholecystectomy: prospective analysis of 386 patients. Hepato‐Gastroenterology 2001;48(41):1271‐4. - PubMed
Perniceni 2001 {published data only}
-
- Perniceni T, Alves A, Levard H, Boudet MJ, Denet C, Gayet B. Can common bile duct lithiasis be removed laparoscopically without external biliary drainage? [Le traitement laparoscopique de la lithiase de la voie biliaire principale sans drainage biliaire externe est‐il possible?]. Gastroenterologie Clinique et Biologique 2001;25(2):149‐53. - PubMed
Phillips 1995 {published data only}
-
- Phillips EH, Liberman M, Carroll BJ, Fallas MJ, Rosenthal R, Hiatt J. Bile duct stones in the laparoscopic era: is pre‐operative sphincterotomy necessary?. Archives of Surgery 1995;130:880‐6. - PubMed
Quershi 1993 {published data only}
-
- Quershi A, Browne A, Leahy AL, Courtney G, Osborne H, Broe PJ, et al. ERCP in the management of patients having laparoscopic cholecystectomy: re‐appraising current indications. Irish Journal of Medical Science 1993;162(12):510‐2. - PubMed
Rabago 2006 {published data only}
-
- Rabago LR, Vincente C, Soler F, Delgado M, Moral I, Guerra I, et al. Two‐stage treatment with preoperative endoscopic retrograde cholangiopancreatography (ERCP) compared with single‐stage treatment with intraoperative ERCP for patients with symptomatic cholelithiasis with possible choledocholithiasis. Endoscopy 2006;38(8):779‐86. - PubMed
Rhodes 1995 {published data only}
-
- Rhodes M, Nathanson L, O'Rourke N, Fielding G. Laparoscopic exploration of the common bile duct: lessons learned from 129 consecutive cases. British Journal of Surgery 1995;82:666‐8. - PubMed
Rieger 1994 {published data only}
-
- Rieger R, Sulzbacher H, Woisetschlager R, Schrenk P, Wayand W. Selective use of ERCP in patients undergoing laparoscopic cholecystectomy. World Journal of Surgery 1994;18(6):900‐4; discussion 904‐5. - PubMed
Rieger 1995 {published data only}
-
- Rieger R, Wayand W. Yield of prospective, noninvasive evaluation of the common bile duct combined with selective ERCP/sphincterotomy in 1390 consecutive laparoscopic cholecystectomy patients. Gastrointestinal Endoscopy 1995;42(1):6‐12. - PubMed
Rijna 2000 {published data only}
-
- Rijna H, Kemps WG, Eijsbouts Q, Meuwissen SG, Cuesta MA. Preoperative ERCP approach to common bile duct stones: results of a selective policy. Digestive Surgery 2000;17(3):229‐33. - PubMed
Robertson 1996 {published data only}
-
- Robertson GS, Jagger C, Johnson PR, Rathbone BJ, Wicks AC, Lloyd DM, et al. Selection criteria for preoperative endoscopic retrograde cholangiopancreatography in the laparoscopic era. Archives of Surgery 1996;131(1):89‐94. - PubMed
Robinson 1995 {published data only}
-
- Robinson G, Hollinshead J, Falk G, Moulton J. Technique and results of laparoscopic choledochotomy for the management of bile duct calculi. Australian and New Zealand Journal of Surgery 1995;65(5):347‐9. - PubMed
Roush 1995 {published data only}
-
- Roush TS, Traverso LW. Management and long‐term follow‐up of patients with positive cholangiograms during laparoscopic cholecystectomy. American Journal of Surgery 1995;169(5):484‐7. - PubMed
Santucci 1996 {published data only}
-
- Santucci L, Natalini G, Sarpi L, Fiorucci S, Solinas A, Morelli A. Selective endoscopic retrograde cholangiography and preoperative bile duct stone removal in patients scheduled for laparoscopic cholecystectomy: a prospective study. American Journal of Gastroenterology 1996;91(7):1326‐30. - PubMed
Sarli 1999 {published data only}
-
- Sarli L, Pietra N, Franze A, Colla G, Costi R, Gobbi S, et al. Routine intravenous cholangiography, selective ERCP, and endoscopic treatment of bile duct stones before laparoscopic cholecystectomy. Gastrointestinal Endoscopy 1999;50(2):200‐8. - PubMed
Schwab 1992 {published data only}
-
- Schwab G, Pointner R, Wetscher G, Glaser K, Foltin E, Bodner E. Treatment of calculi of the common bile duct. Surgery, Gynecology and Obstetrics 1992;175(2):115‐20. - PubMed
Seo 2000 {published data only}
-
- Seo DW. Prospective analysis of endoscopic papillary balloon dilatation and endoscopic sphincterotomy for removal of common bile duct stones. Gastrointestinal Endoscopy 2000;52(1):140‐2. - PubMed
Stoker 1995 {published data only}
-
- Stoker ME. Common bile duct exploration in the era of laparoscopic surgery. Archives of Surgery 1995;130(3):265‐9. - PubMed
Sugiyama 1999 {published data only}
-
- Sugiyama M, Izumisato Y, Hatano N, Mori T, Atomi Y. Management of unsuspected common bile duct stones found during laparoscopic cholecystectomy by means of transcystic catheter placement and papillary dilation. Gastrointestinal Endoscopy 1999;50(6):837‐40. - PubMed
Sungler 1993 {published data only}
-
- Sungler P, Heinerman PM, Mayer F, Boeckl O. Laparoscopic cholecystectomy in cholecysto‐choledocholithiasis. "Therapeutic splitting" or conventional surgical procedure?. Chirurg 1993;64(12):1012‐5; discussion 1016‐7. - PubMed
Sungler 1997 {published data only}
-
- Sungler P, Holzinger J, Heinerman PM, Waclawiczek HW, Boeckl O. Preoperative therapeutic splitting [Preoperatives therapeutisches splitting]. Zentralblatt fur Chirurgie 1997;122(12):1083‐7. - PubMed
Tham 1998 {published data only}
-
- Tham TC, Lichtenstein DR, Vandervoort J, Wong RC, Brooks D, Dam J, et al. Role of endoscopic retrograde cholangiopancreatography for suspected choledocholithiasis in patients undergoing laparoscopic cholecystectomy. Gastrointestinal Endoscopy 1998;47(1):50‐6. - PubMed
Trias 1997 {published data only}
-
- Trias M, Targarona EM, Ros E, Bordas JM, Perez Ayuso RM, Balague C, et al. Prospective evaluation of a minimally invasive approach for treatment of bile‐duct calculi in the high‐risk patient. Surgical Endoscopy 1997;11(6):632‐5. - PubMed
Trondsen 1995 {published data only}
-
- Trondsen E, Edwin B, Reiertsen O, Fagertun H, Rosseland AR. Selection criteria for endoscopic retrograde cholangiopancreaticography (ERCP) in patients with gallstone disease. World Journal of Surgery 1995;19(6):852‐7. - PubMed
Turcu 1997 {published data only}
-
- Turcu F. A minimally invasive approach in choledocholithiasis [Abordul miniinvaziv al litiazei de cale biliara principala]. Chirurgia (Bucuresti) 1997;92(3):145‐53. - PubMed
Waage 2003 {published data only}
-
- Waage A, Stromberg C, Leijonmarck CE, Arvidsson D. Long‐term results from laparoscopic common bile duct exploration. Surgical Endoscopy and Other Interventional Techniques 2003;17(8):1181‐5. - PubMed
Welbourn 1995 {published data only}
Wenner 2005 {published data only}
-
- Wenner DE, Whitwam P, Rosser J, Hashmi S, Wenner DE. A stone extraction facilitation device to achieve an improved technique for performing LCBDE. Surgical Endoscopy and Other Interventional Techniques 2005;19(1):120‐5. - PubMed
Widdison 1994 {published data only}
-
- Widdison AL, Longstaff AJ, Armstrong CP. Combined laparoscopic and endoscopic treatment of gallstones and bile duct stones: a prospective study. British Journal of Surgery 1994;81(4):595‐7. - PubMed
Wilson 1993 {published data only}
-
- Wilson TG, Jeans PL, Anthony A, Cox MR, Toouli J. Laparoscopic cholecystectomy and management of choledocholithiasis. Australian and New Zealand Journal of Surgery 1993;63(6):443‐50. - PubMed
Worthley 1989 {published data only}
-
- Worthley CS, Watts JM, Toouli J. Common duct exploration or endoscopic sphincterotomy for choledocholithiasis?. Australian and New Zealand Journal of Surgery 1989;59(3):209‐15. - PubMed
Zargar 2002 {published data only}
-
- Zagar SA, Javid G, Khan, et al. Endoscopic sphincterotomy in the management of the commmon bile duct stones: results in 170 patients. JK Practitioner 2002;9:20‐3.
Additional references
Begg 1996
-
- Begg C, Cho M, Eastwood S, Horton R, Moher D, Olkin I, et al. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA 1996;276:637‐9. - PubMed
Brok 2008
-
- Brok J, Thorlund K, Gluud C, Wetterslev J. Trial sequential analysis reveals insufficient information size and potentially false positive results in many meta‐analyses. Journal of Clinical Epidemiology 2008;61:763‐9. - PubMed
Brok 2009
-
- Brok J, Thorlund K, Wetterslev J, Gluud C. Apparently conclusive meta‐analyses may be inconclusive‐‐Trial sequential analysis adjustment of random error risk due to repetitive testing of accumulating data in apparently conclusive neonatal meta‐analyses. International Journal of Epidemiology 2009;38(1):287‐98. - PubMed
Clayton 2006
-
- Clayton ES, Connor S, Alexakis N, Leandros E. Meta‐analysis of endoscopy and surgery versus surgery alone for common bile duct stones with the gallbladder in situ. British Journal of Surgery 2006;93(10):1185‐91. - PubMed
Coelho‐Prabhu 2013
Collins 2004
CTU 2011
-
- Copenhagen Trial Unit. TSA ‐ Trial Sequential Analysis. http://ctu.dk/tsa/ 2011 (accessed 5 July 2013).
Egger 1997
Fletcher 1994
-
- Fletcher DR. Changes in the practice of biliary surgery and ERCP during the introduction of laparoscopic cholecystectomy to Australia: their possible significance. Australian and New Zealand Journal of Surgery 1994;64(2):75‐80. - PubMed
Gluud 2013
-
- Gluud C, Nikolova D, Klingenberg SL, Alexakis N, Als‐Nielsen B, Colli A, et al. Cochrane Hepato‐Biliary Group. About The Cochrane Collaboration (Cochrane Review Groups (CRGs)). 2013, Issue 7. Art. No.: LIVER.
Gurusamy 2009
-
- Gurusamy KS, Gluud C, Nikolova D, Davidson BR. Assessment of risk of bias in randomized clinical trials in surgery. British Journal of Surgery 2009;96(4):342‐9. - PubMed
Hozo 2005
Kjaergard 2001
-
- Kjaergard LL, Villumsen J, Gluud C. Reported methodologic quality and discrepancies between large and small randomized trials in meta‐analyses. Annals of Internal Medicine 2001;135(11):982‐9. - PubMed
Ko 2002
-
- Ko CW, Lee SP. Epidemiology and natural history of common bile duct stones and prediction of disease. Review. Gastrointestinal Endoscopy 2002;56(6 Suppl):S165‐S169. [MEDLINE: ] - PubMed
Lundh 2012
Macaskill 2001
-
- Macaskill P, Walter SD, Irwig L. A comparision of methods to detect publication bias in meta‐analysis. Statistics in Medicine 2001;20(4):641‐54. - PubMed
Mercer 2007
Moher 1998
-
- Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta‐analyses?. Lancet 1998;352(9128):609‐13. - PubMed
Neoptolemos 1989
-
- Neoptolemos JP, Rowley S. Advantages of nonsurgical treatment of bile duct stones. Hepato‐Gastroenterology 1989;36(5):313‐6. - PubMed
Newell 1992
-
- Newell DJ. Intention‐tot‐treat analysis: implications for quantitative and qualitative research. International Journal of Epidemiology 1992;21(5):837‐41. - PubMed
RevMan 2012 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012.
Rojas‐Ortega 2003
-
- Rojas‐Ortega S, Arizpe‐Bravo D, Marín López ER, Cesin‐Sánchez R, Roman GR, Gómez C. Transcystic common bile duct exploration in the management of patients with choledocholithiasis. Journal of Gastrointestinal Surgery 2003;7(4):492‐6. - PubMed
Savovic 2012a
-
- Savovic J, Jones HE, Altman DG, Harris RJ, Jüni P, Pildal J, et al. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Health Technology Assessment 2012;16(35):1‐82. - PubMed
Savovic 2012b
-
- Savovic J, Jones HE, Altman DG, Harris RJ, Jüni P, Pildal J, et al. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Annals of Internal Medicine 2012;157(6):429‐38. - PubMed
Schulz 1995
-
- Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995;273(5):408‐12. - PubMed
Soltan 2000
-
- Soltan, Kow, Toouli. A simple scoring system for predicting bile duct stones in patients with cholelithiasis. Journal of Gastrointestinal Surgery 2001;5(4):434‐7. - PubMed
SPIRIT 2013
Stinton 2012
Tazuma 2006
-
- Tazuma S. Epidemiology, pathogenesis, and classification of biliary stones (common bile duct and intrahepatic). Best Practice and Research Clinical Gastroenterology 2006;20:1075‐83. - PubMed
Thorlund 2009
-
- Thorlund K, Devereaux PJ, Wetterslev J, Guyatt G, Ioannidis JP, Thabane L, et al. Can trial sequential monitoring boundaries reduce spurious inferences from meta‐analyses. International Journal of Epidemiology 2009;38(1):276‐86. - PubMed
Thorlund 2010
Thorlund 2011
-
- Thorlund K, Engstrøm J, Wetterslev J, Brok J, Imberger G, Gluud C. User manual forTrial Sequential Analysis (TSA). http://ctu.dk/tsa/files/tsa_manual.pdf 2011 (accessed 5 July 2013).
Wetterslev 2008
-
- Wetterslev J, Thorlund K, Brok J, Gluud C. Trial sequential analysis may establish when firm evidence is reached in cumulative meta‐analysis. Journal of Clinical Epidemiology 2008;61(1):64‐75. - PubMed
Wetterslev 2009
Williams 2008
-
- Williams EJ, Green J, Beckingham I, Parks R, Martin D, Lombard M. Guidelines on the management of common bile duct stones (CBDS). Gut 2008;57:1004‐21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical