

Gradual lengthening of the ulna in patients with multiple hereditary exostoses with a dislocated radial head
- PMID: 24339304
- PMCID: PMC3874895
- DOI: 10.3349/ymj.2014.55.1.178
Gradual lengthening of the ulna in patients with multiple hereditary exostoses with a dislocated radial head
Abstract
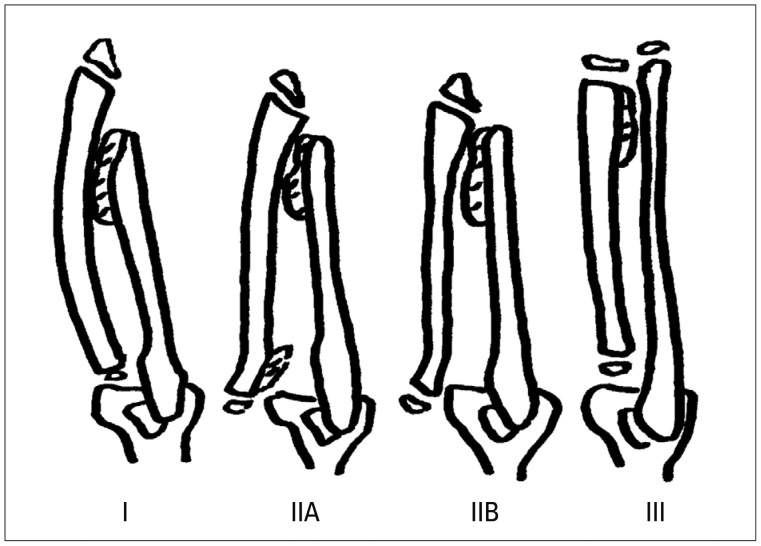
Purpose: Multiple hereditary exostoses of the forearm typically form in the distal ulna, causing disturbances in the growth of the ulna and functional disability. Multiple hereditary exostoses inhibit the growth of the ulna, leading to an acquisition of a varus deformity in the radius, which sometimes leads to dislocation of the radial head, the development of limitations in the pronation-supination of the forearm, and cosmetic problems.
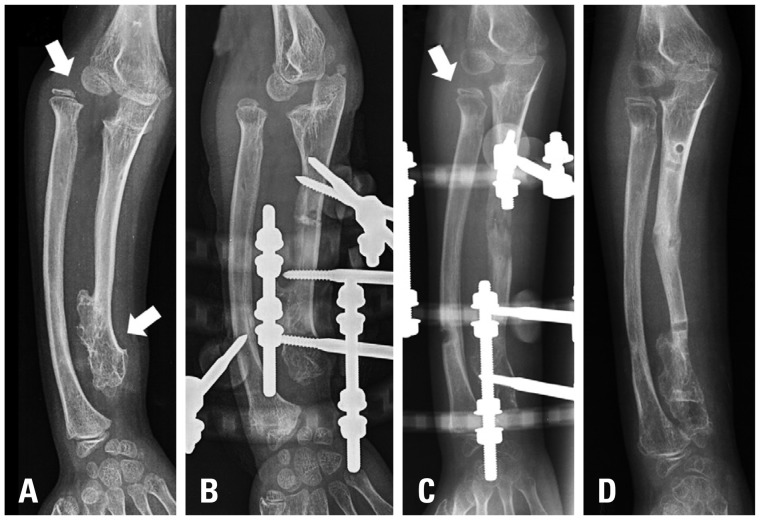
Materials and methods: We retrospectively reviewed the cases of four patients who had deformities of the forearm with radial head dislocation associated with multiple hereditary exostoses, and evaluated the radiologic and clinical results of excision of the osteochondromas from the distal ulna and gradual ulnar lengthening with an Ilizarov external fixator.
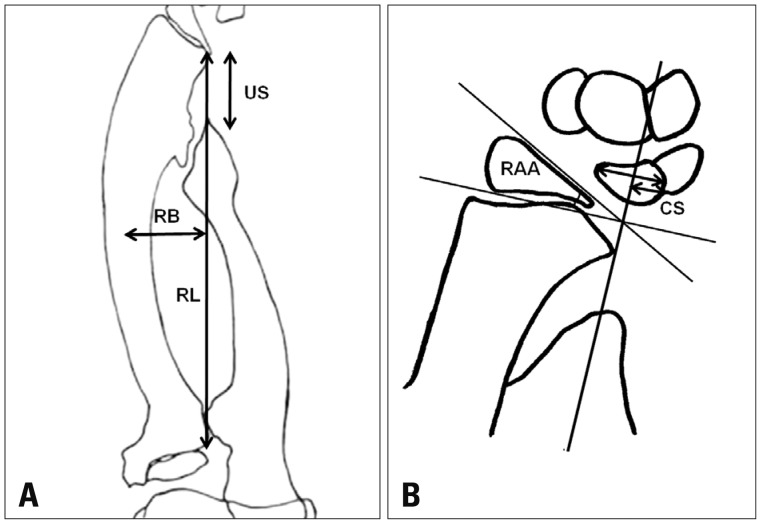
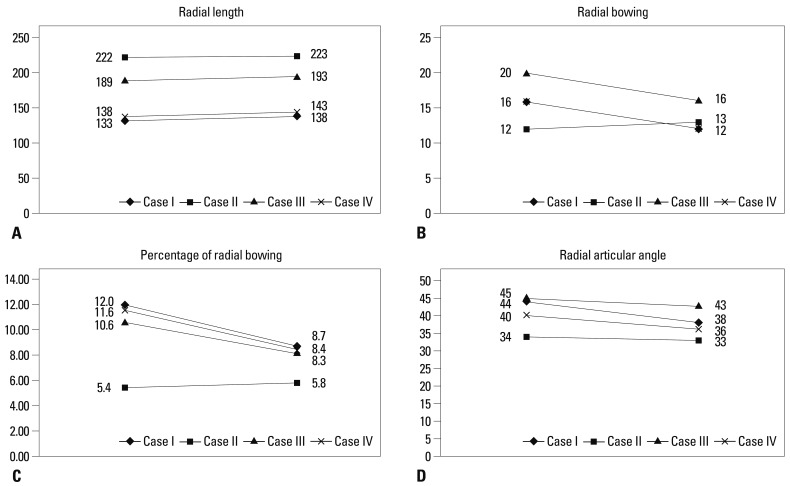
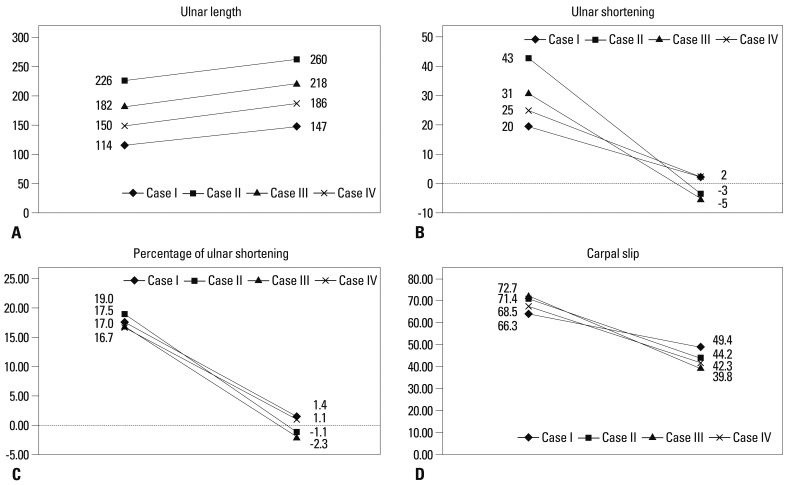
Results: Good clinical and radiological results were obtained after a mean follow-up of 25 months. At the most recent follow-up, radial bowing, ulnar shortening, carpal slip, and the pronation/supination arch of the forearm had improved. There was little change in terms of preoperative radial articular angle and the flexion/extension arch of the elbow by the most recent follow-up.
Conclusion: Treatment of four forearms from four patients by excision of osteochondromas and gradual lengthening of the ulna with an Ilizarov external fixator spontaneously reduced dislocations of the radial heads without the need for any additional operative intervention. All patients were satisfied with the final results.
Keywords: Ilizarov external fixator; Multiple hereditary exostosis; gradual lengthening.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
Similar articles
-
Gradual ulnar lengthening by an Ilizarov ring fixator for correction of Masada IIb forearm deformity without tumor excision in hereditary multiple exostosis: preliminary results.J Pediatr Orthop B. 2019 Jan;28(1):67-72. doi: 10.1097/BPB.0000000000000514. J Pediatr Orthop B. 2019. PMID: 29995654
-
Reconstruction of forearm deformity by distraction osteogenesis in children with relative shortening of the ulna due to multiple cartilaginous exostosis.J Pediatr Orthop. 2011 Jun;31(4):393-401. doi: 10.1097/BPO.0b013e31821a5e27. J Pediatr Orthop. 2011. PMID: 21572277
-
Modified Ilizarov technique for the treatment of forearm deformities in multiple cartilaginous exostoses: case series and literature review.J Hand Surg Eur Vol. 2013 Mar;38(3):288-96. doi: 10.1177/1753193412450651. Epub 2012 Jun 19. J Hand Surg Eur Vol. 2013. PMID: 22719009 Review.
-
Ulnar lengthening for children with forearm deformity from hereditary multiple exostoses: a retrospective study from a tertiary medical center.BMC Pediatr. 2024 Sep 16;24(1):585. doi: 10.1186/s12887-024-05063-9. BMC Pediatr. 2024. PMID: 39285333 Free PMC article.
-
Timing of forearm deformity correction in a child with multiple hereditary exostosis.Am J Orthop (Belle Mead NJ). 2014 Sep;43(9):422-5. Am J Orthop (Belle Mead NJ). 2014. PMID: 25251529 Review.
Cited by
-
Management of Forearm Deformity by Limb Reconstruction System in Children with Multiple Exostosis - A case Report.J Orthop Case Rep. 2020 Sep;10(6):14-17. doi: 10.13107/jocr.2020.v10.i06.1856. J Orthop Case Rep. 2020. PMID: 33489961 Free PMC article.
-
Gradual ulnar lengthening in Masada type I/IIb deformity in patients with hereditary multiple osteochondromas: a retrospective study with a mean follow-up of 4.2 years.J Orthop Surg Res. 2020 Dec 9;15(1):594. doi: 10.1186/s13018-020-02137-z. J Orthop Surg Res. 2020. PMID: 33298090 Free PMC article.
-
Hinge positioning method of Ilizarov apparatus in correcting radial head luxation caused by multiple hereditary exostoses.Jt Dis Relat Surg. 2022;33(1):40-50. doi: 10.52312/jdrs.2022.502. Epub 2022 Mar 28. Jt Dis Relat Surg. 2022. PMID: 35361079 Free PMC article.
-
Ulnar lengthening in the treatment of forearm deformity caused by hereditary multiple exostoses in children.World J Orthop. 2025 Jul 18;16(7):108319. doi: 10.5312/wjo.v16.i7.108319. eCollection 2025 Jul 18. World J Orthop. 2025. PMID: 40709297 Free PMC article. Review.
-
Limb Length Discrepancy and Angular Deformity due to Benign Bone Tumors and Tumor-like Lesions.J Am Acad Orthop Surg Glob Res Rev. 2021 Mar 10;5(3):e00214. doi: 10.5435/JAAOSGlobal-D-20-00214. J Am Acad Orthop Surg Glob Res Rev. 2021. PMID: 33720060 Free PMC article.
References
-
- Solomon L. Bone growth in diaphysial aclasis. J Bone Joint Surg Br. 1961;43-B:700–716. - PubMed
-
- Wood VE, Sauser D, Mudge D. The treatment of hereditary multiple exostosis of the upper extremity. J Hand Surg Am. 1985;10:505–513. - PubMed
-
- Schmale GA, Conrad EU, 3rd, Raskind WH. The natural history of hereditary multiple exostoses. J Bone Joint Surg Am. 1994;76:986–992. - PubMed
-
- Shapiro F, Simon S, Glimcher MJ. Hereditary multiple exostoses. Anthropometric, roentgenographic, and clinical aspects. J Bone Joint Surg Am. 1979;61:815–824. - PubMed
-
- Masada K, Tsuyuguchi Y, Kawai H, Kawabata H, Noguchi K, Ono K. Operations for forearm deformity caused by multiple osteochondromas. J Bone Joint Surg Br. 1989;71:24–29. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
