

Autoimmune encephalitis: A potentially reversible cause of status epilepticus, epilepsy, and cognitive decline
- PMID: 24339583
- PMCID: PMC3841604
- DOI: 10.4103/0972-2327.120476
Autoimmune encephalitis: A potentially reversible cause of status epilepticus, epilepsy, and cognitive decline
Abstract
Objectives: To review clinical characteristics and response to immunomodulation therapy in autoimmune encephalitis presenting with status epilepticus (SE), epilepsy, and cognitive decline.
Design: Observational, prospective case series.
Setting: All India Institute of Medical Sciences, New Delhi, India.
Materials and methods: Prospective analysis of 15 patients, who presented with SE, epilepsy, cognitive decline, and other neurological symptoms with positive autoantibodies. Demographic and clinical characteristics were recorded. Brain magnetic resonance imaging (MRI), cerebrospinal-fluid analysis (CSF), and tumor screening were done periodically. Treatment received and responses (categorized as per patients and treating doctor's information) were noted.
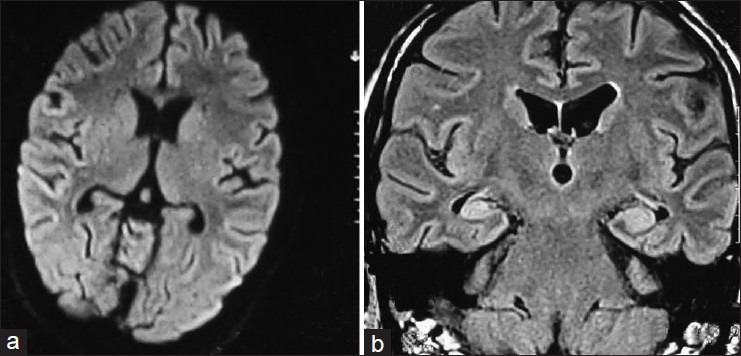
Results: There were 15 (males = 10) patients of autoimmune encephalitis. The mean age of presentation was 24 years (range: 2-64 years). The most common onset was subacute (64%) and four (29%) patients presented as SE. Predominant clinical presentations were seizures (100%) almost of every semiology. CSF was done in 10 patients; it was normal in 60%. Brain MRI was done in all patients, in six (40%) it was normal, six (40%) showed T2W and FLAIR hyperintensities in bilateral limbic areas. Antibodies found were the N-methyl-D-aspartate receptor antibody in seven (50%), voltage-gated potassium channel antibody in five (36%), two of antiglutamic acid decarboxylase, and one patient with double stranded DNA (dsDNA) antibodies. None showed evidence of malignancy. Patients received immunotherapy, either steroids, intravenous immunoglobulin, or both. Follow-up showed significant improvement in majority of cases, neither further seizures nor relapse in nine (67%) cases. One death occurred, due to delayed presentation.
Conclusions: Uncommon but potentially reversible causes of SE, epilepsy, and cognitive decline may be immune-related and high index of suspicion will prevent missing the diagnosis.
Keywords: Autoimmune encephalitis; cognitive decline; drug refractory epilepsy; seizures; status epilepticus.
Conflict of interest statement
Figures
References
-
- Tüzün E, Dalmau J. Limbic encephalitis and variants: Classification, diagnosis and treatment. Neurologist. 2007;13:261–71. - PubMed
-
- Vincent A, Buckley C, Schott JM, Baker I, Dewar BK, Detert N, et al. Potassium channel antibody-associated encephalopathy: A potentially immunotherapy-responsive form of limbic encephalitis. Brain. 2004;127(Pt 3):701–12. - PubMed
-
- Thieben MJ, Lennon VA, Boeve BF, Aksamit AJ, Keegan M, Vernino S. Potentially reversible autoimmune limbic encephalitis with neuronal potassium channel antibody. Neurology. 2004;62:1177–82. - PubMed
-
- Pittock SJ, Yoshikawa H, Ahlskog JE, Tisch SH, Benarroch EE, Kryzer TJ, et al. Glutamic acid decarboxylase autoimmunity with brainstem, extrapyramidal, and spinal cord dysfunction. Mayo Clin Proc. 2006;81:1207–14. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
