

Immunoglobulin g4 non-related sclerosing disease with intracardiac mass mimicking mitral stenosis: case report
- PMID: 24339717
- PMCID: PMC3857383
- DOI: 10.3346/jkms.2013.28.12.1830
Immunoglobulin g4 non-related sclerosing disease with intracardiac mass mimicking mitral stenosis: case report
Abstract
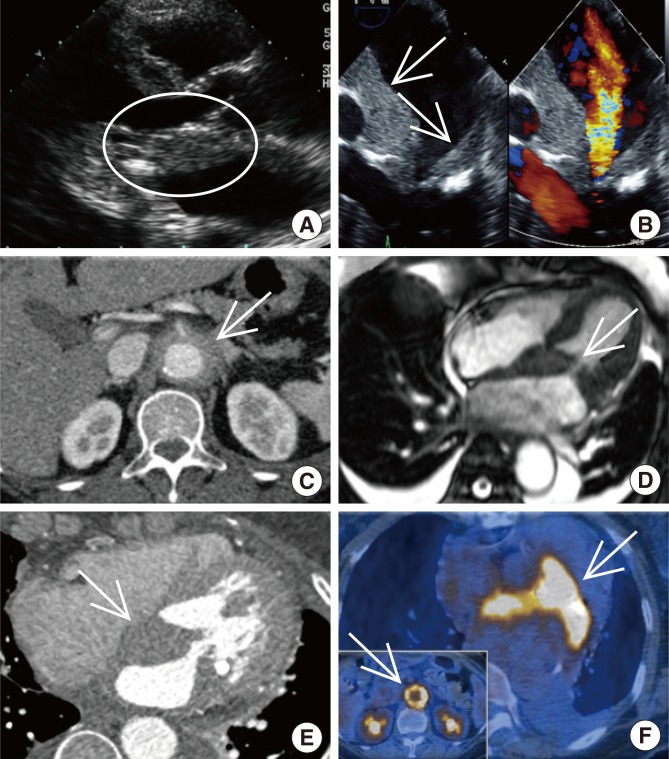
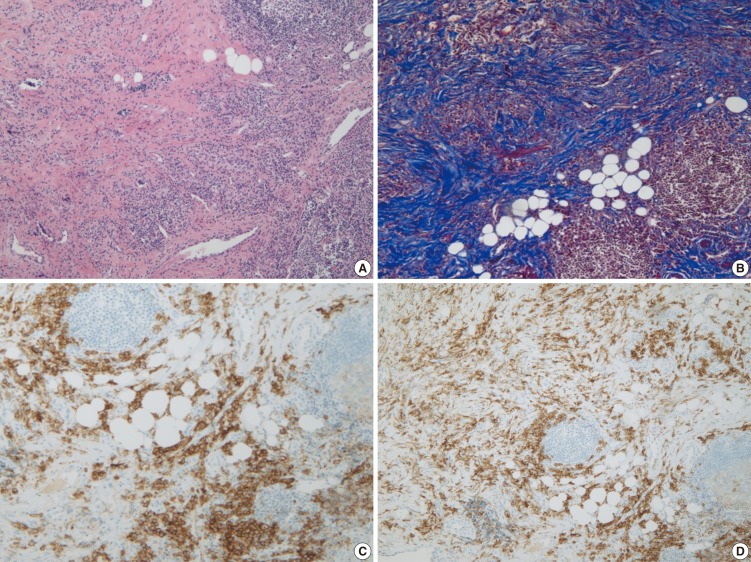
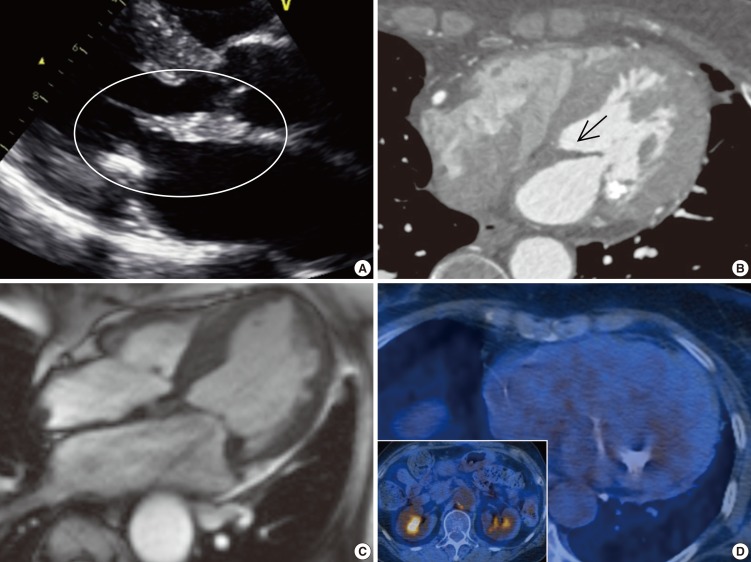
The cardiovascular system may be one of the target organs of both immunoglobulin G4 related and non-related systemic multifocal fibrosclerosis. We present a case of IgG4 non-related systemic multifocal fibrosclerosis mimicking mitral stenosis on echocardiography. For a more detailed differential diagnosis, we used multimodal imaging techniques. After surgical biopsy around the abdominal aortic area in the retroperitoneum, histological examination revealed IgG4 non-related systemic multifocal fibrosclerosis. We describe the multimodal imaging used to diagnose IgG4 non-related systemic multifocal fibrosclerosis and a positive response to steroid treatment. There have been no previous case reports of IgG4 non-related systemic multifocal fibrosclerosis with intracardiac involvement. Here, we report a case of IgG4 non-related systemic multifocal fibrosclerosis mimicking mitral stenosis.
Keywords: Immunoglobulin G4 Non-Related Sclerosing Disease; Left Atrium Mass; Mitral Valve Stenosis; Periaortitis.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
