

Evidence for the therapeutic efficacy of either mild hypothermia or oxygen radical scavengers after repetitive mild traumatic brain injury
- PMID: 24341607
- PMCID: PMC3967419
- DOI: 10.1089/neu.2013.3181
Evidence for the therapeutic efficacy of either mild hypothermia or oxygen radical scavengers after repetitive mild traumatic brain injury
Abstract
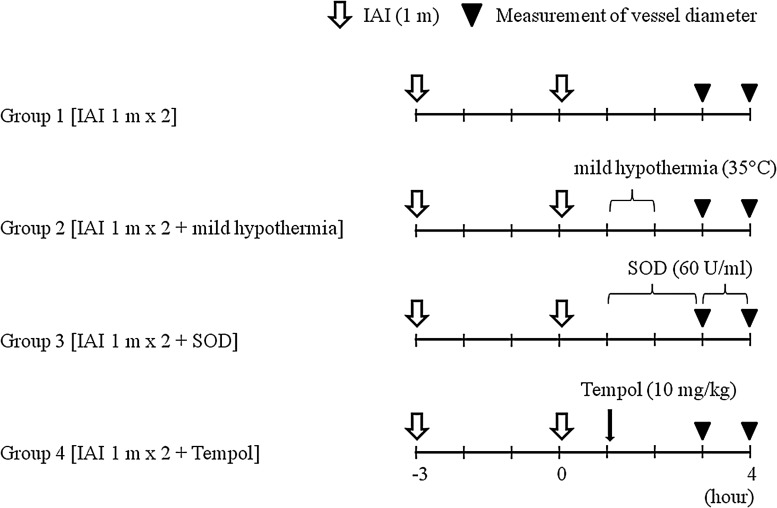
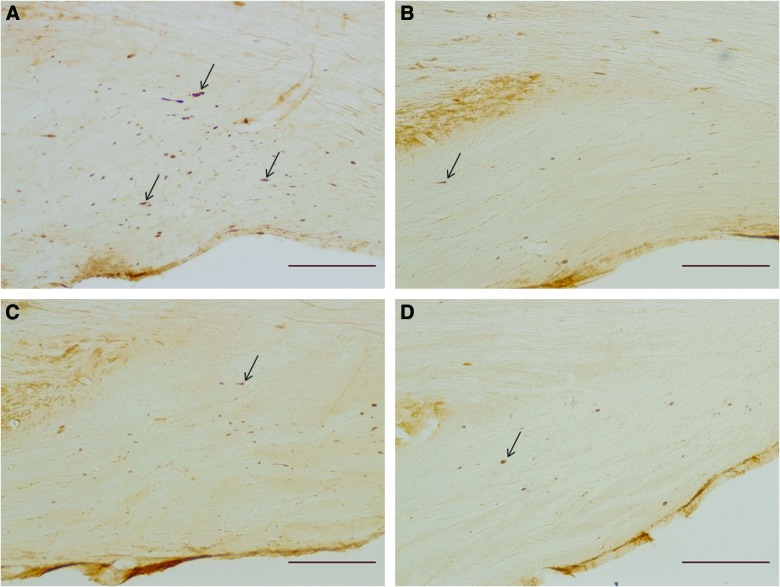
Repetitive brain injury, particularly that occurring with sporting-related injuries, has recently garnered increased attention in both the clinical and public settings. In the laboratory, we have demonstrated the adverse axonal and vascular consequences of repetitive brain injury and have demonstrated that moderate hypothermia and/or FK506 exerted protective effects after repetitive mild traumatic brain injury (mTBI) when administered within a specific time frame, suggesting a range of therapeutic modalities to prevent a dramatic exacerbation. In this communication, we revisit the utility of targeted therapeutic intervention to seek the minimal level of hypothermia needed to achieve protection while probing the role of oxygen radicals and their therapeutic targeting. Male Sprague-Dawley rats were subjected to repetitive mTBI by impact acceleration injury. Mild hypothermia (35 °C, group 2), superoxide dismutase (group 3), and Tempol (group 4) were employed as therapeutic interventions administered 1 h after the repetitive mTBI. To assess vascular function, cerebral vascular reactivity to acetylcholine was evaluated 3 and 4 h after the repetitive mTBI, whereas to detect the burden of axonal damage, amyloid precursor protein (APP) density in the medullospinal junction was measured. Whereas complete impairment of vascular reactivity was observed in group 1 (without intervention), significant preservation of vascular reactivity was found in the other groups. Similarly, whereas remarkable increase in the APP-positive axon was observed in group 1, there were no significant increases in the other groups. Collectively, these findings indicate that even mild hypothermia or the blunting free radical damage, even when performed in a delayed period, is protective in repetitive mTBI.
Figures



References
-
- Allen G.V., Gerami D., and Esser M.J. (2000). Conditioning effects of repetitive mild neurotrauma on motor function in an animal model of focal brain injury. Neuroscience 99, 93–105 - PubMed
-
- Laurer H., Bareyre F.M., Lee V.M.Y.C., Trojanowski J.Q., Longhi L., Hoover R., Saatman K.E., Raghupathi R., Hoshino S., Grady M.S., and McIntosh T.K. (2001). Mild head injury increasing the brain's vulnerability to a second concussive impact. J. Neurosurg. 95, 859–870 - PubMed
-
- Collins M.W., Lovell M.R., Iverson G.L., Cantu R.C., Maroon J.C., and Field M. (2002). Cumulative effects of concussion in high school athletes. Neurosurgery 51, 1175–1181 - PubMed
-
- Raghpathi R., Mehr M.F., Helfaer M.A., and Margulies S.S. (2004). Traumatic axonal injury is exacerbated following repetitive closed head injury in the neonatal pig. J. Neurotrauma 21, 307–316 - PubMed
-
- Moser R.S., Schatz P., and Jordan B.D. (2005). Prolonged effects of concussion in high school athletes. Neurosurgery 57, 300–306 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
