

Longitudinal patterns of anxiety from childhood to adulthood: the Great Smoky Mountains Study
- PMID: 24342383
- PMCID: PMC3939681
- DOI: 10.1016/j.jaac.2013.09.017
Longitudinal patterns of anxiety from childhood to adulthood: the Great Smoky Mountains Study
Abstract
Objective: The aims of this study were 2-fold: to provide a brief introduction to the prospective longitudinal Great Smoky Mountains Study and review recent findings; and to use this sample to conduct an epidemiologic analysis of common childhood anxiety disorders.
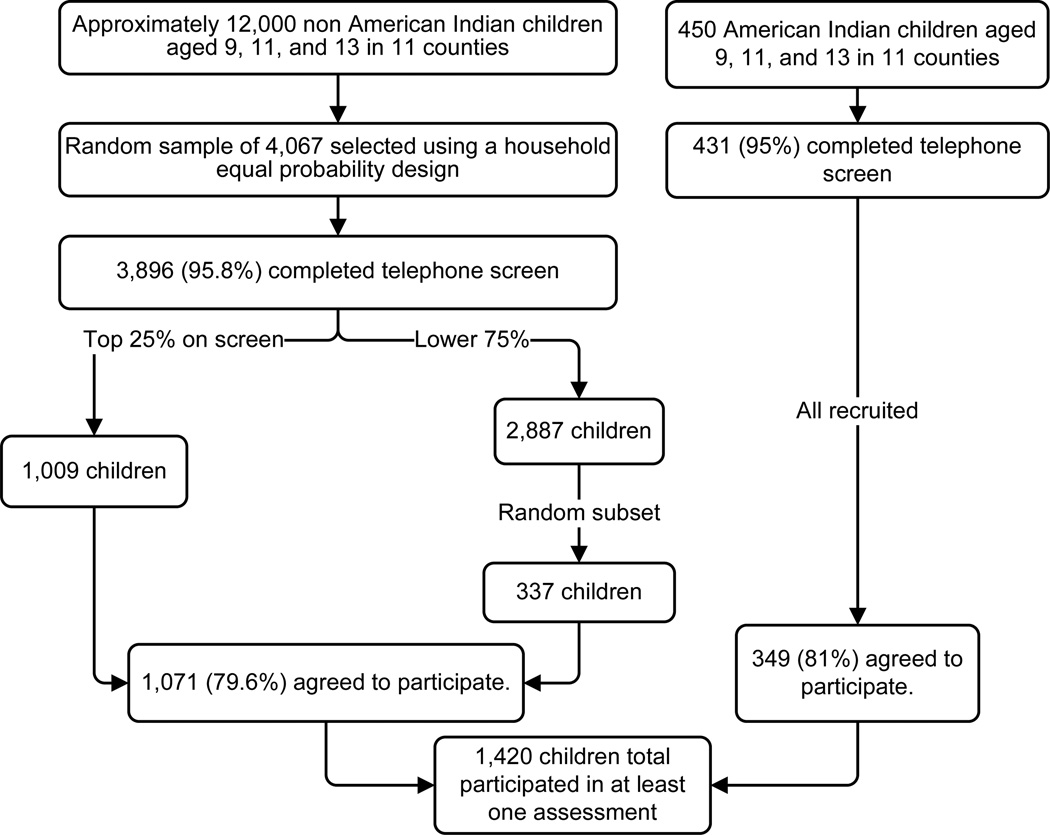
Method: The population-based Great Smoky Mountains Study assessed 1,420 participants from 11 counties in the southeastern United States up to 11 times between ages 9 and 26 years with the structured Child and Adolescent Psychiatric Assessment and its upward extension, the Young Adult Psychiatric Assessment.
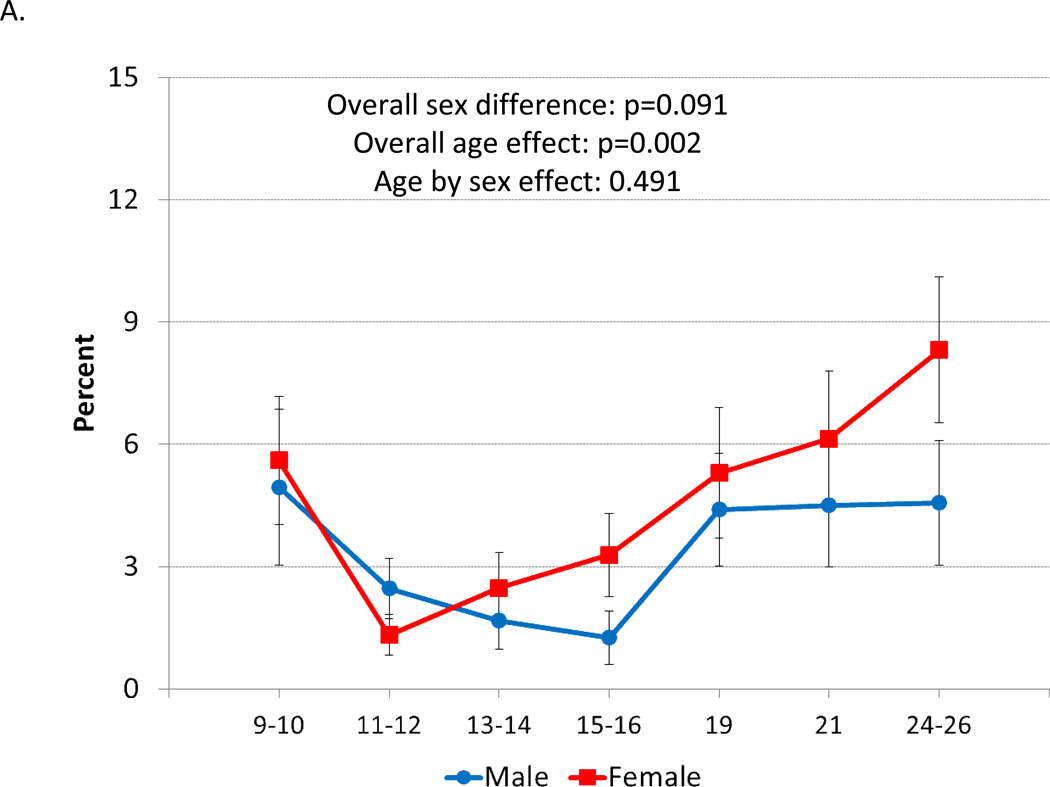
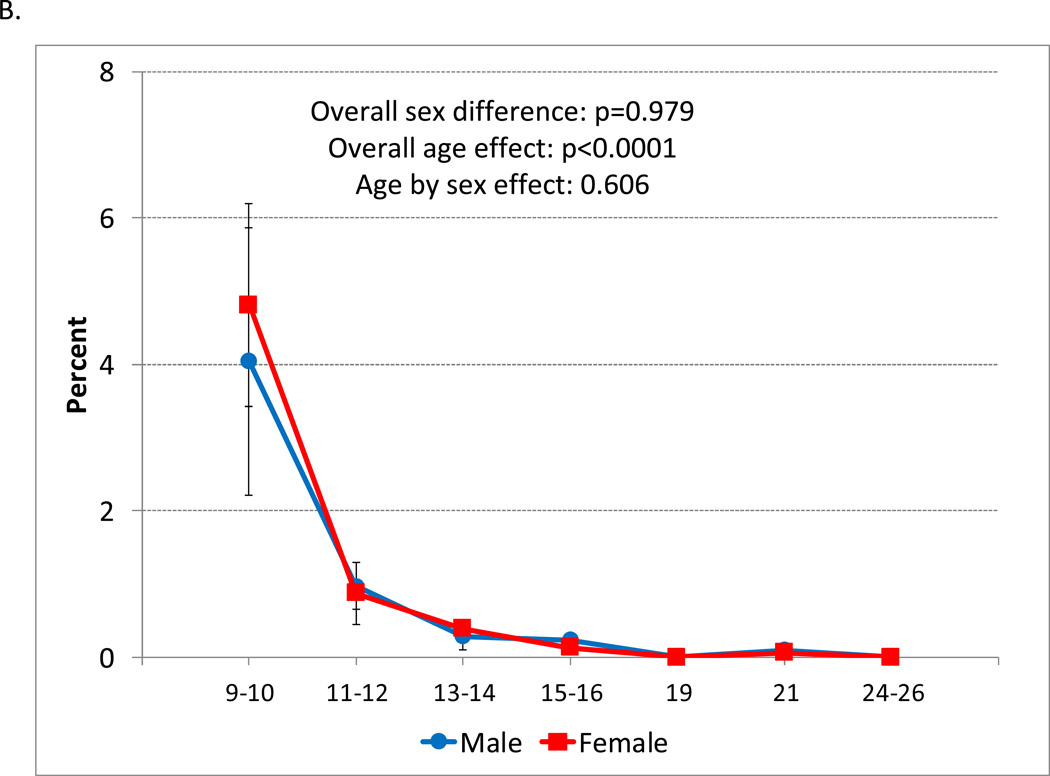
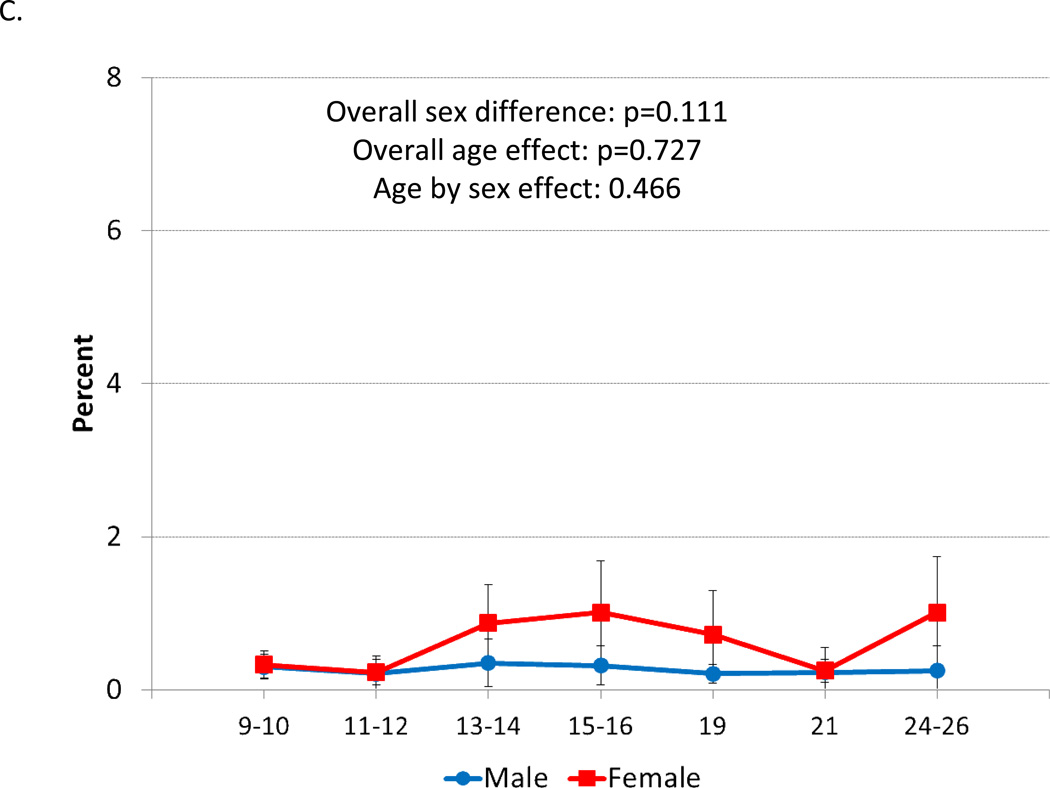
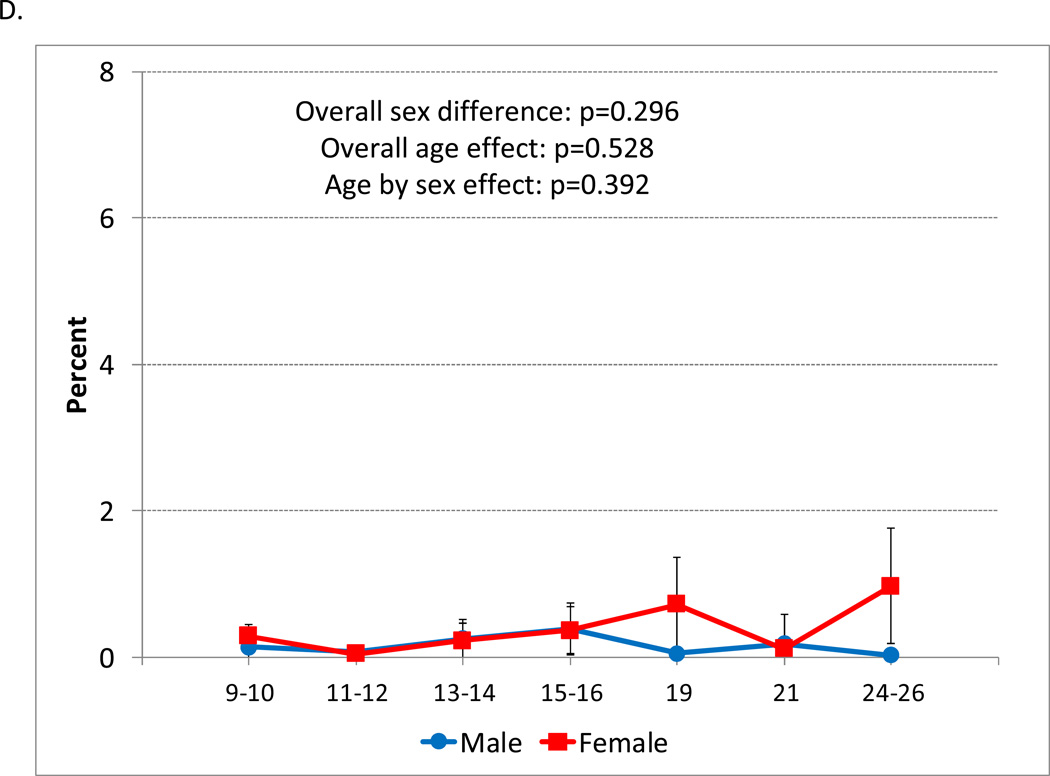
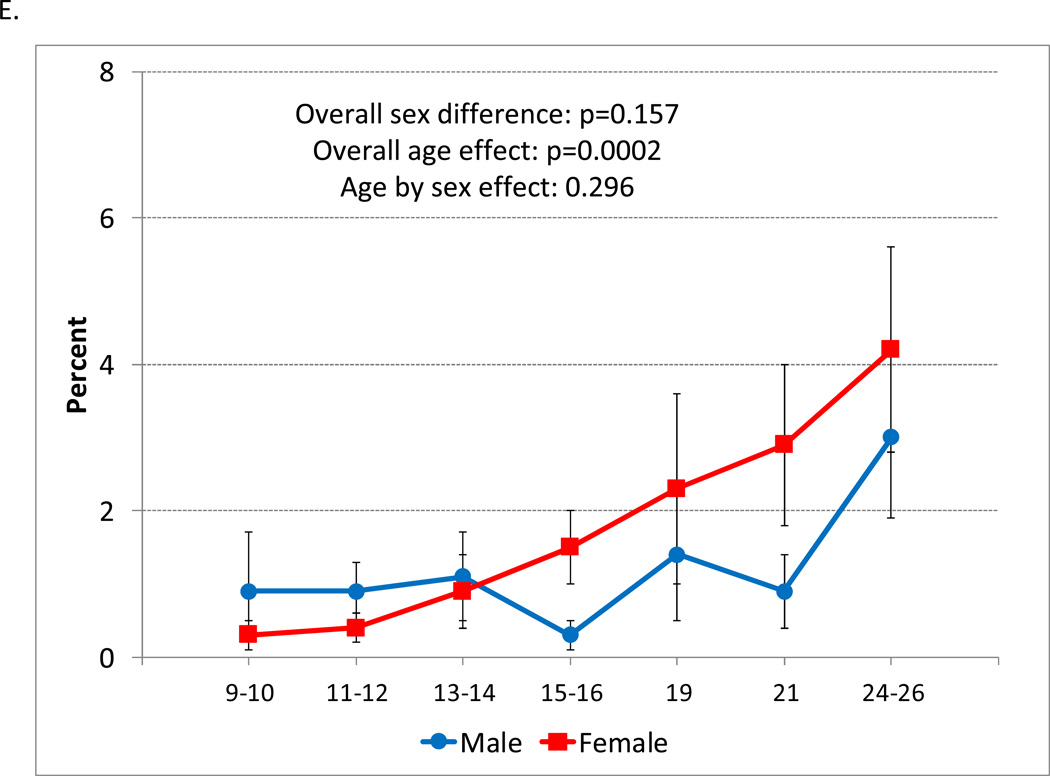
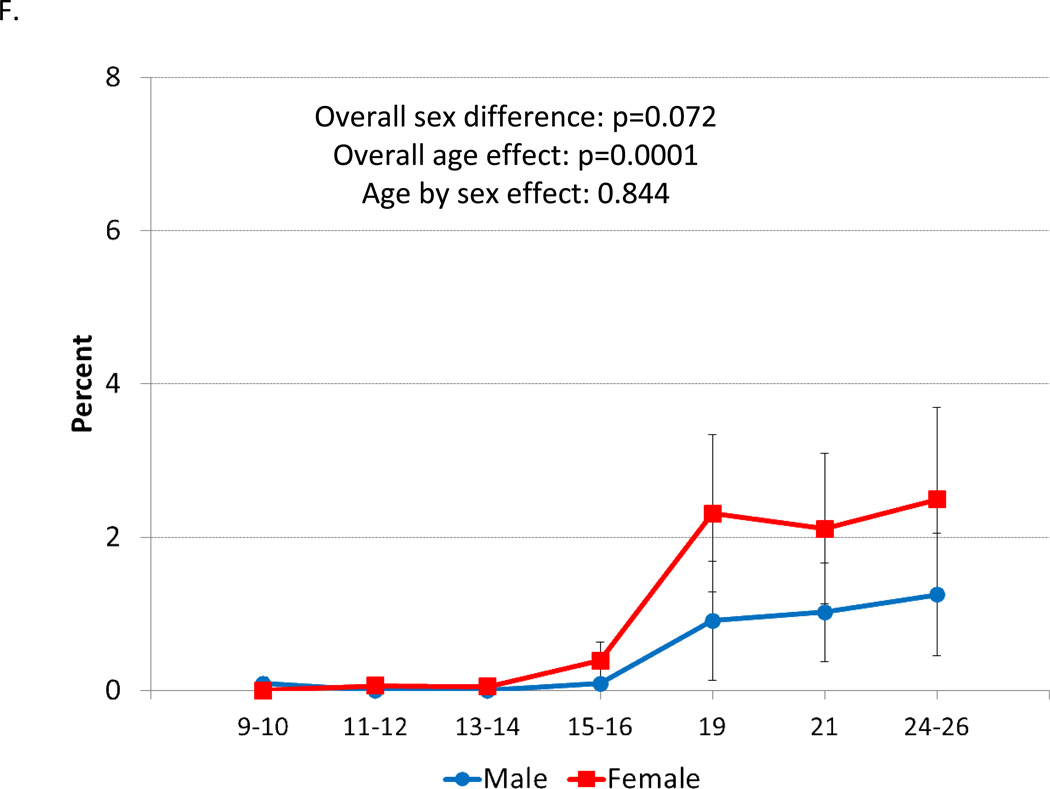
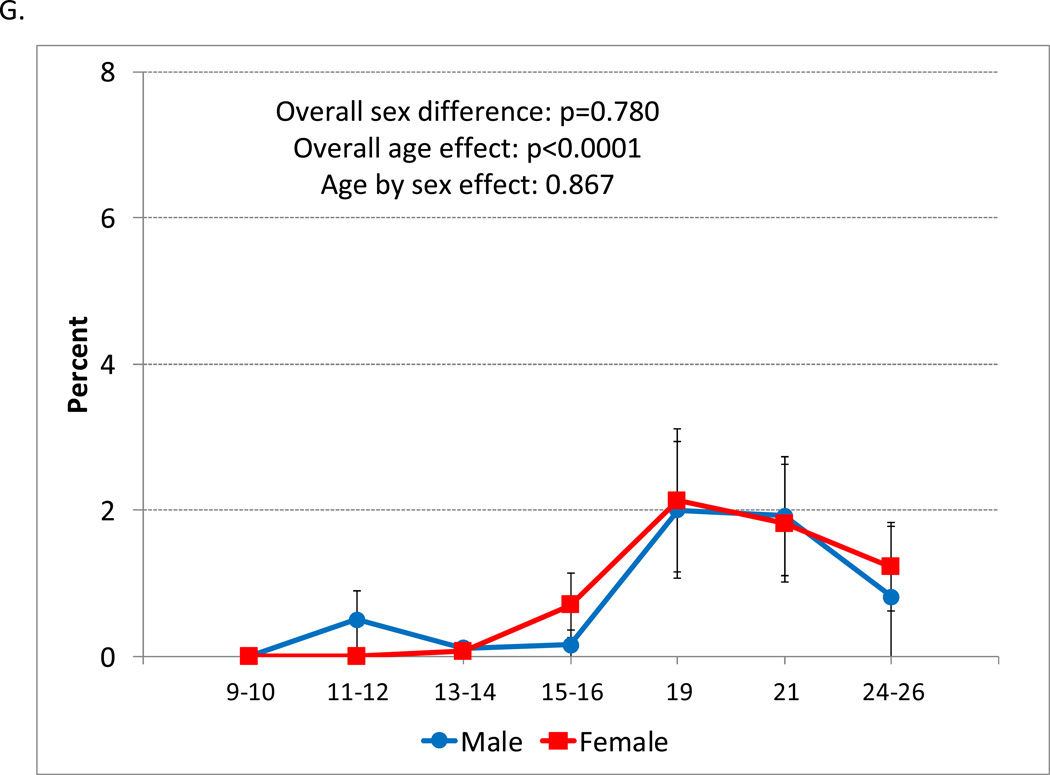
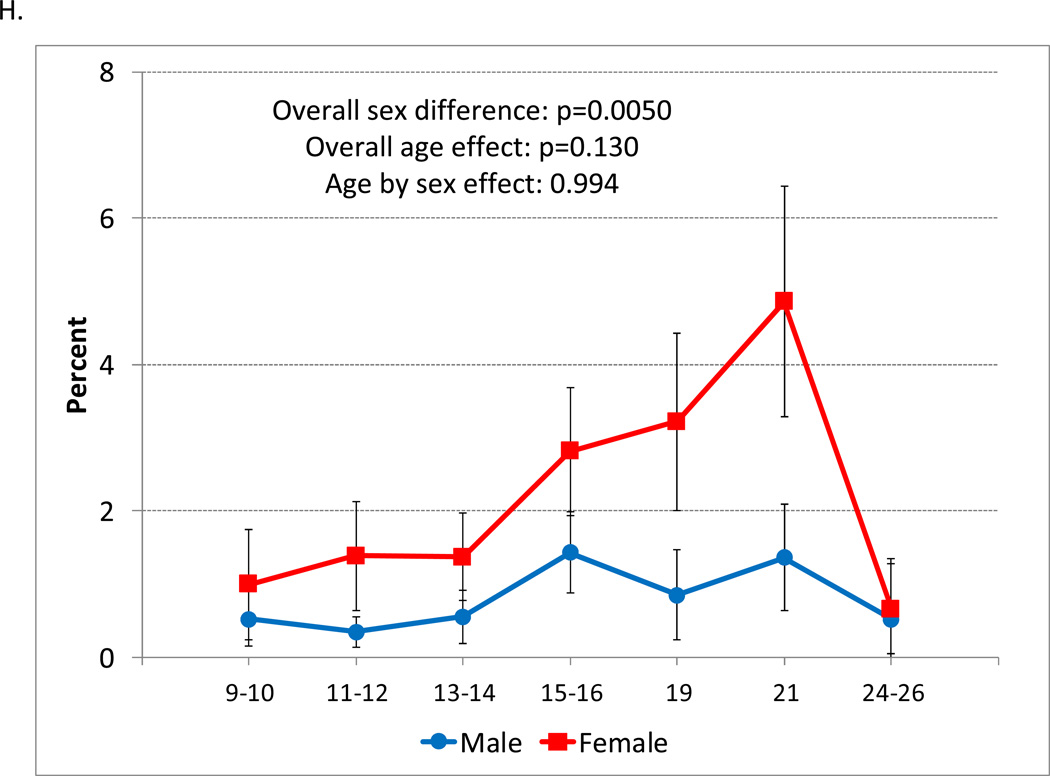
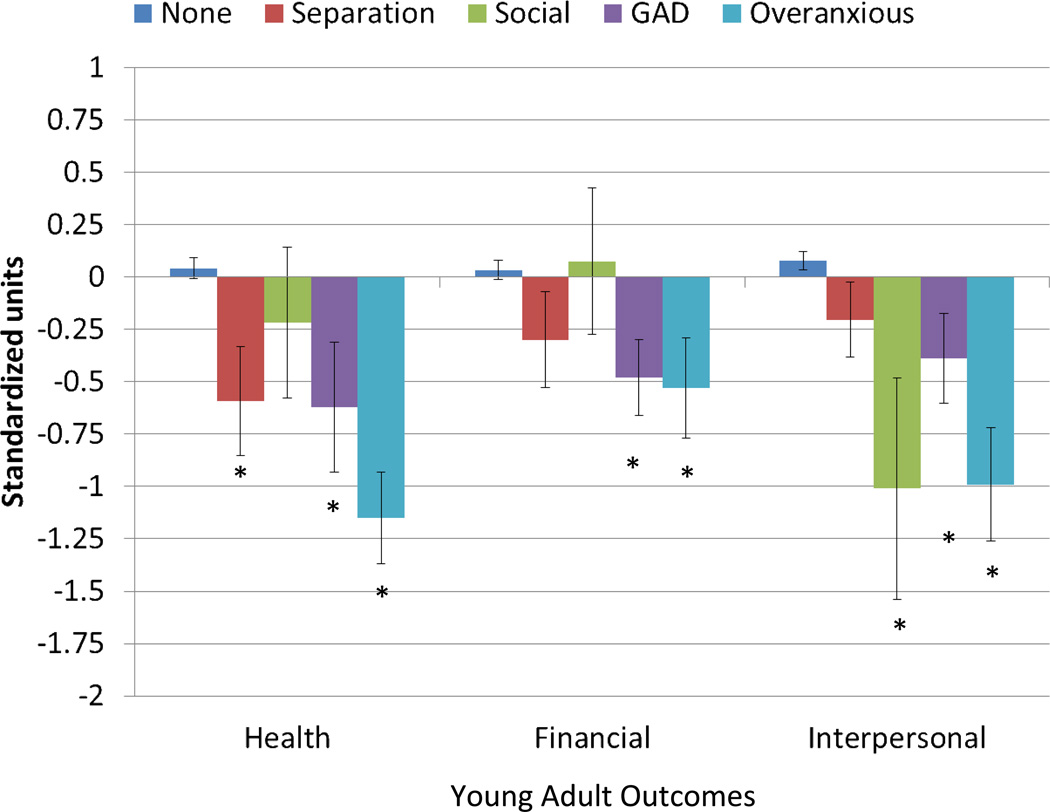
Results: The U-shaped age prevalence curve for any anxiety disorder was the product of high levels of childhood separation anxiety and adult panic, agoraphobia, and generalized anxiety. More than 1 in 5 subjects met criteria for an anxiety disorder by early adulthood. In terms of cumulative comorbidity, there was evidence of overlap between anxiety disorders, but the level of overlap was generally consistent with what is seen among other common childhood disorders. All childhood anxiety disorders were associated with adverse functioning in at least 1 young adult functional domain, with the poorest outcomes for childhood generalized anxiety and DSM-III-R overanxious disorder.
Conclusion: Clinically significant anxiety is a common mental health problem to have had by adulthood. There was little evidence to support the consolidation of anxiety disorders, and some evidence to justify reintroduction of DSM-III-R overanxious disorder. The transition to young adulthood appears to be a key period for understanding the development of common adult anxiety disorders such as panic and agoraphobia.
Keywords: anxiety; comorbidity; development; epidemiology; longitudinal.
Copyright © 2014 American Academy of Child and Adolescent Psychiatry. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Rutter M. Isle of Wight revisited. Journal of the American Academy of Child and Adolescent Psychiatry. 1989;28:633–653. - PubMed
-
- Costello EJ, Angold A, Burns B, et al. The Great Smoky Mountains Study of Youth: Goals, designs, methods, and the prevalence of DSM-III-R disorders. Archives of General Psychiatry. 1996;53:1129–1136. - PubMed
-
- Berkson J. Limitations of the application of fourfold table analysis to hospital data. Biometrics Bulletin. 1946;2:47–52. - PubMed
-
- Rothman KJ, Greenland S. Modern Epidemiology. Second ed. Philadelphia: Lippincott-Raven; 1998.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
