

Bicuspid aortic cusp fusion morphology alters aortic three-dimensional outflow patterns, wall shear stress, and expression of aortopathy
- PMID: 24345403
- PMCID: PMC3946057
- DOI: 10.1161/CIRCULATIONAHA.113.003026
Bicuspid aortic cusp fusion morphology alters aortic three-dimensional outflow patterns, wall shear stress, and expression of aortopathy
Abstract
Background: Aortic 3-dimensional blood flow was analyzed to investigate altered ascending aorta (AAo) hemodynamics in bicuspid aortic valve (BAV) patients and its association with differences in cusp fusion patterns (right-left, RL versus right-noncoronary, RN) and expression of aortopathy.
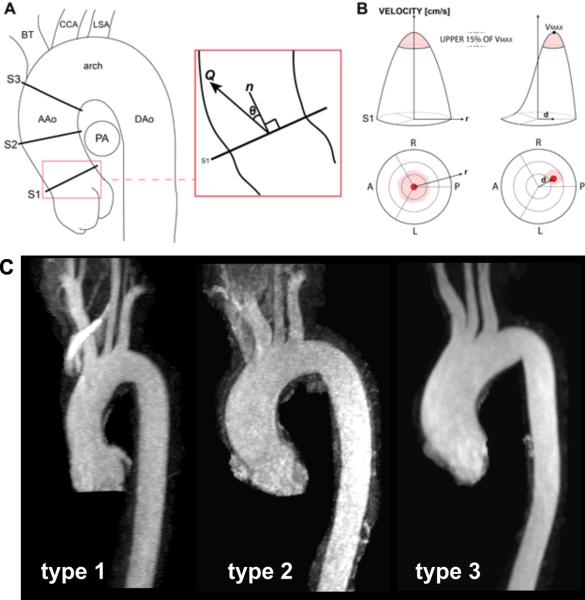
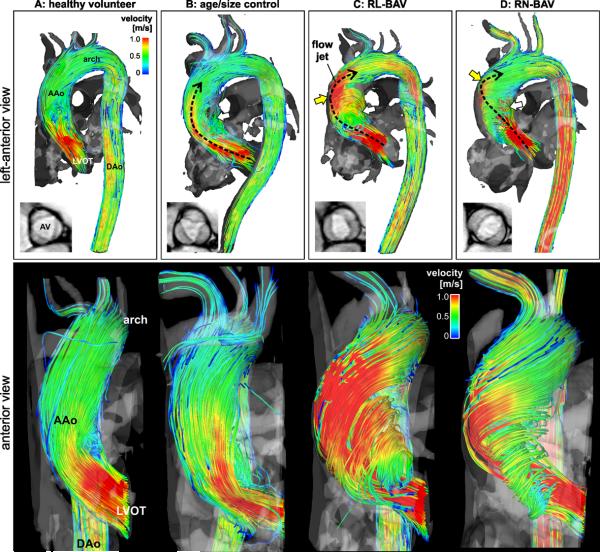
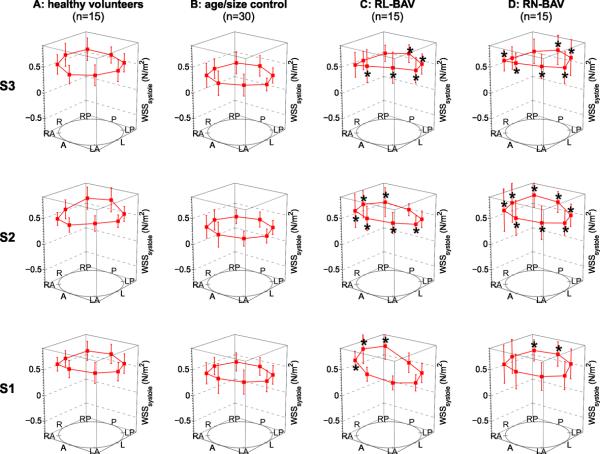
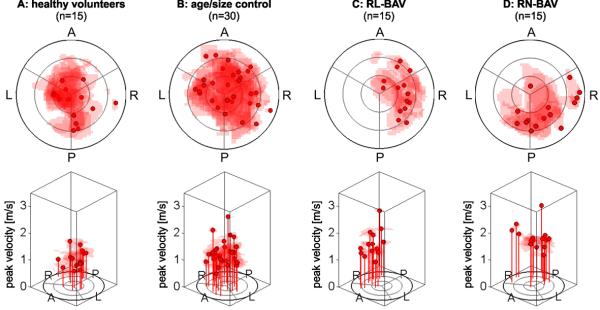
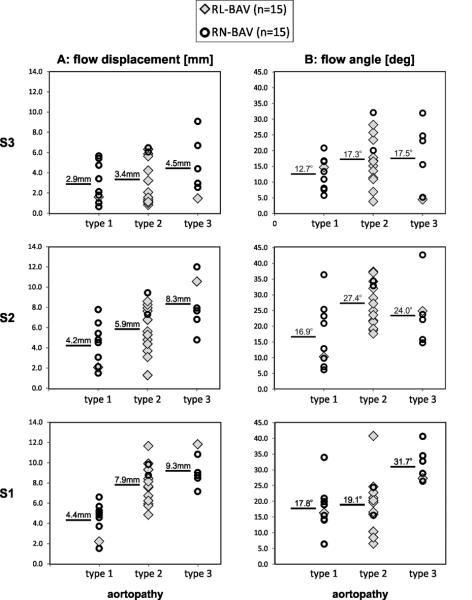
Methods and results: Four-dimensional flow MRI measured in vivo 3-dimensional blood flow in the aorta of 75 subjects: BAV patients with aortic dilatation stratified by leaflet fusion pattern (n=15 RL-BAV, mid AAo diameter=39.9±4.4 mm; n=15 RN-BAV, 39.6±7.2 mm); aorta size controls with tricuspid aortic valves (n=30, 41.0±4.4 mm); healthy volunteers (n=15, 24.9±3.0 mm). Aortopathy type (0-3), systolic flow angle, flow displacement, and regional wall shear stress were determined for all subjects. Eccentric outflow jet patterns in BAV patients resulted in elevated regional wall shear stress (P<0.0125) at the right-anterior walls for RL-BAV and right-posterior walls for RN-BAV in comparison with aorta size controls. Dilatation of the aortic root only (type 1) or involving the entire AAo and arch (type 3) was found in the majority of RN-BAV patients (87%) but was mostly absent for RL-BAV patients (87% type 2). Differences in aortopathy type between RL-BAV and RN-BAV patients were associated with altered flow displacement in the proximal and mid AAo for type 1 (42%-81% decrease versus type 2) and distal AAo for type 3 (33%-39% increase versus type 2).
Conclusions: The presence and type of BAV fusion was associated with changes in regional wall shear stress distribution, systolic flow eccentricity, and expression of BAV aortopathy. Hemodynamic markers suggest a physiological mechanism by which the valve morphology phenotype can influence phenotypes of BAV aortopathy.
Keywords: aortic diseases; bicuspid aortic valve; hemodynamics; magnetic resonance imaging.
Figures
Comment in
-
Nature versus nurture in bicuspid aortic valve aortopathy: more evidence that altered hemodynamics may play a role.Circulation. 2014 Feb 11;129(6):622-4. doi: 10.1161/CIRCULATIONAHA.113.007282. Epub 2013 Dec 17. Circulation. 2014. PMID: 24345404 No abstract available.
-
Letter by Hope et al regarding article, "Bicuspid aortic cusp fusion morphology alters aortic three-dimensional outflow patterns, wall shear stress, and expression of aortopathy".Circulation. 2014 Nov 4;130(19):e170. doi: 10.1161/CIRCULATIONAHA.114.008824. Circulation. 2014. PMID: 25366842 No abstract available.
-
Response to letter regarding article, "Bicuspid aortic cusp fusion morphology alters aortic three-dimensional outflow patterns, wall shear stress, and expression of aortopathy".Circulation. 2014 Nov 4;130(19):e171. doi: 10.1161/CIRCULATIONAHA.114.010928. Circulation. 2014. PMID: 25366843 Free PMC article. No abstract available.
References
-
- Fedak PWM, Verma S, David TE, Leask RL, Weisel RD, Butany J. Clinical and pathophysiological implications of a bicuspid aortic valve. Circulation. 2002;106:900–904. - PubMed
-
- Michelena HI, Khanna AD, Mahoney D, Margaryan E, Topilsky Y, Suri RM, Eidem B, Edwards WD, Sundt TM, 3rd, Enriquez-Sarano M. Incidence of aortic complications in patients with bicuspid aortic valves. JAMA. 2011;306:1104–1112. - PubMed
-
- Rudolph AM. Congenital diseases of the heart. Wiley-Blackwell; 2009. Bicuspid aortic valve and aortic stenosis; pp. 225–256.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
