

Male urethral strictures and their management
- PMID: 24346008
- PMCID: PMC4123447
- DOI: 10.1038/nrurol.2013.275
Male urethral strictures and their management
Abstract
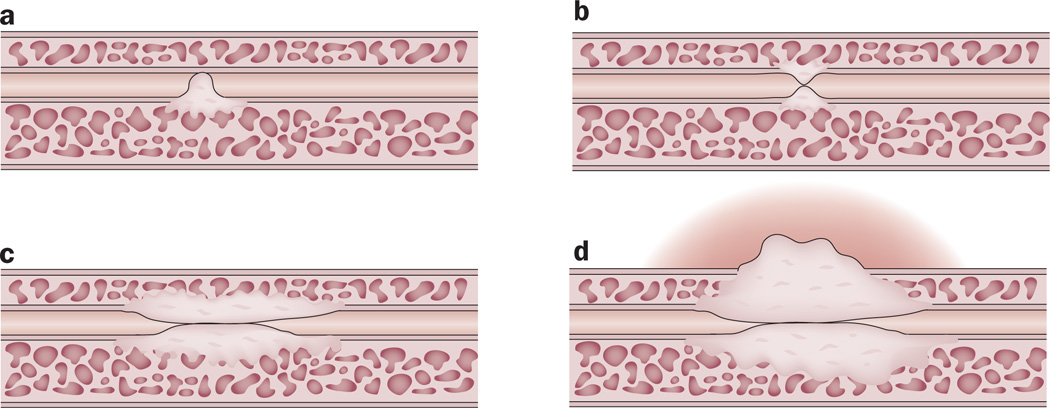
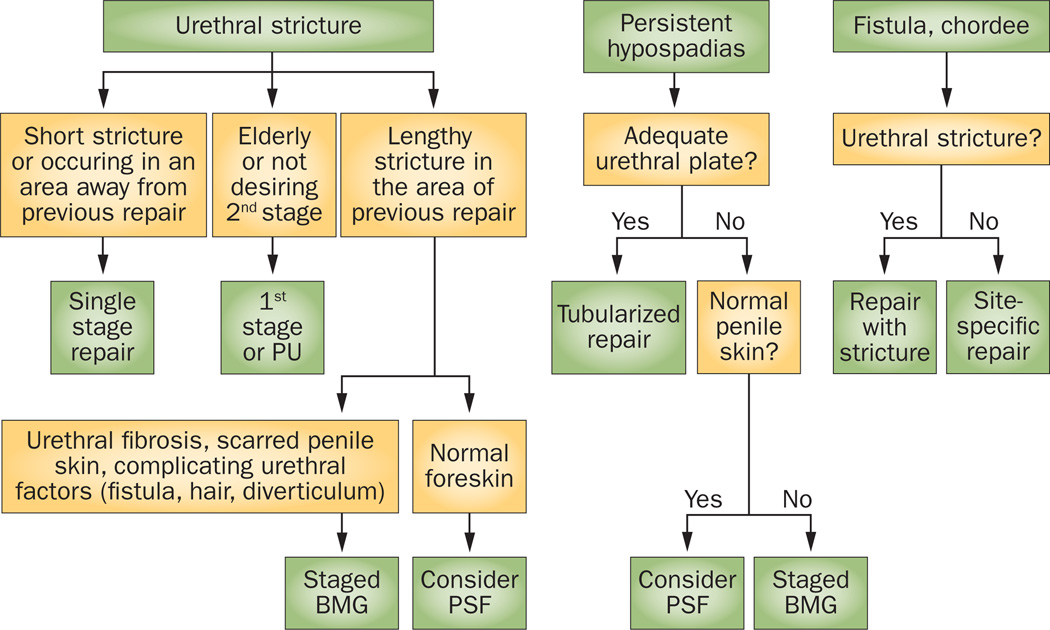
Male urethral stricture disease is prevalent and has a substantial impact on quality of life and health-care costs. Management of urethral strictures is complex and depends on the characteristics of the stricture. Data show that there is no difference between urethral dilation and internal urethrotomy in terms of long-term outcomes; success rates range widely from 8-80%, with long-term success rates of 20-30%. For both of these procedures, the risk of recurrence is greater for men with longer strictures, penile urethral strictures, multiple strictures, presence of infection, or history of prior procedures. Analysis has shown that repeated use of urethrotomy is not clinically effective or cost-effective in these patients. Long-term success rates are higher for surgical reconstruction with urethroplasty, with most studies showing success rates of 85-90%. Many techniques have been utilized for urethroplasty, depending on the location, length, and character of the stricture. Successful management of urethral strictures requires detailed knowledge of anatomy, pathophysiology, proper patient selection, and reconstructive techniques.
Figures
References
-
- Santucci RA, Joyce GF, Wise M. Male urethral stricture disease. J. Urol. 2007;177:1667–1674. - PubMed
-
- Palminteri E, et al. Contemporary urethral stricture characteristics in the developed world. Urology. 2013;81:191–197. - PubMed
-
- Chambers RM, Baitera B. The anatomy of the urethral stricture. Br. J. Urol. 1977;49:545–551. - PubMed
-
- Singh M, Blandy JP. The pathology of urethral stricture. J. Urol. 1976;115:673–676. - PubMed
-
- Cavalcanti A, Costa WS, Baskin LS, McAninch JA, Sampaio FJB. A morphometric analysis of bulbar urethral strictures. BJU Int. 2007;100:397–402. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
